Large Acute Intracerebral Hemorrhage: Clinical Presentation, Diagnostic Challenges, Management, and Outcomes - A Case Report
OthersPage Navigation
Abstract
Large acute intracerebral hemorrhage (ICH) is a neurological emergency associated with high morbidity and mortality, depending on hematoma volume, location, intraventricular extension, and the patient’s baseline neurological status. Rapid clinical deterioration may occur due to mass effect, raised intracranial pressure, and secondary brain injury. We report a confirmed case of large spontaneous intracerebral hemorrhage in a middle-aged male presenting with sudden-onset headache, vomiting, and rapidly progressive neurological deficits. This case highlights the clinical presentation, diagnostic challenges, neuroimaging evaluation, acute medical and neurosurgical management, critical care considerations, and clinical outcomes. The report emphasizes the importance of early recognition, prompt neuroimaging, aggressive blood pressure control, management of raised intracranial pressure, timely neurosurgical consultation, and structured rehabilitation to optimize neurological recovery and reduce mortality.
Introduction
Intracerebral hemorrhage accounts for approximately 10–15% of all strokes and is associated with disproportionately high mortality and long-term disability. The most common etiologies include chronic hypertension, cerebral amyloid angiopathy, anticoagulant or antiplatelet use, vascular malformations, and coagulopathies. Large-volume hemorrhages are particularly devastating due to mass effect, midline shift, and risk of herniation. Clinical presentation is often abrupt, with severe headache, vomiting, altered sensorium, focal neurological deficits, and rapid neurological decline. Early adherence to evidence-based stroke and neurocritical care protocols, urgent neuroimaging, and multidisciplinary management are critical determinants of outcome. This case report describes the presentation, diagnostic workup, management strategy, and outcome of a patient with large acute intracerebral hemorrhage.
Case Report
Patient History
A 56-year-old man was brought to the emergency department with sudden-onset severe headache, repeated vomiting, and right-sided weakness that developed over 1 hour. The patient had a 10-year history of poorly controlled hypertension and irregular antihypertensive use. There was no history of recent trauma, seizures, or loss of consciousness prior to presentation. He was not on anticoagulant or antiplatelet therapy. There was no prior history of stroke or known bleeding disorders.
Clinical Examination
On arrival, the patient was drowsy but arousable to painful stimuli. Vital signs showed blood pressure 210/120 mmHg, heart rate 96/min, respiratory rate 22/min, and oxygen saturation 95% on room air. Neurological examination revealed Glasgow Coma Scale (GCS) score of 10/15 (E2V3M5). There was dense right-sided hemiplegia (power 0/5 in both upper and lower limbs), right facial droop, and aphasia. Pupils were equal and reactive. Fundoscopy showed features suggestive of hypertensive retinopathy. No signs of external trauma were present. Cardiovascular and respiratory examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
The differential diagnoses included:
• Large acute intracerebral hemorrhage
• Acute ischemic stroke with hemorrhagic transformation
• Ruptured arteriovenous malformation
• Intracranial tumor with hemorrhage
• Cerebral venous sinus thrombosis with hemorrhagic infarction
Investigations
Urgent non-contrast computed tomography (CT) of the brain demonstrated a large left basal ganglia hemorrhage measuring approximately 6.2 × 4.8 × 4.5 cm with surrounding edema, intraventricular extension into the lateral ventricle, and a 7 mm midline shift.
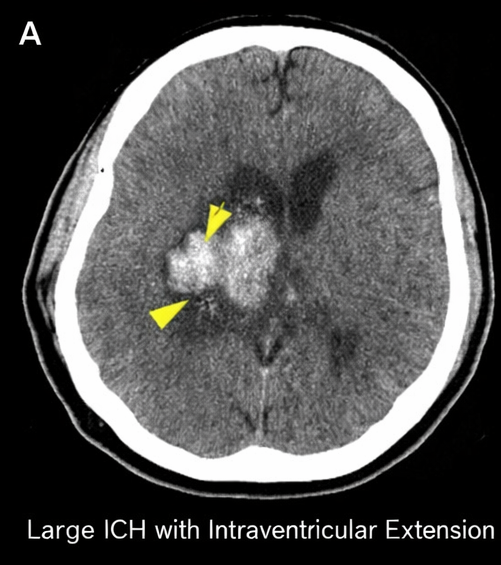
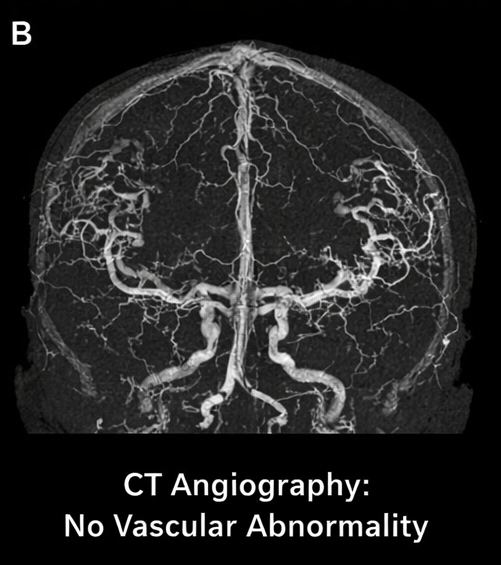
There was effacement of the ipsilateral lateral ventricle and early signs of raised intracranial pressure. CT angiography did not reveal any underlying vascular malformation or aneurysm.
Baseline laboratory investigations showed elevated blood pressure-related end-organ changes, mild leukocytosis, and normal coagulation profile. Serum electrolytes and renal function were within normal limits.
Diagnosis
Based on clinical presentation and neuroimaging findings, a diagnosis of large acute spontaneous intracerebral hemorrhage involving the left basal ganglia with intraventricular extension and mass effect was established, most likely secondary to chronic uncontrolled hypertension.
Management and Outcome
Management Strategy
The patient was managed in a neurocritical care unit. Initial management followed standard acute stroke and intracranial hemorrhage protocols. Airway protection was ensured, and supplemental oxygen was provided. Aggressive blood pressure control was initiated with intravenous antihypertensive agents to maintain systolic blood pressure below 140 mmHg. Measures to control raised intracranial pressure included head-end elevation, osmotherapy with hypertonic saline/mannitol, and careful fluid management. Anticoagulants and antiplatelets were avoided. Seizure prophylaxis was initiated.
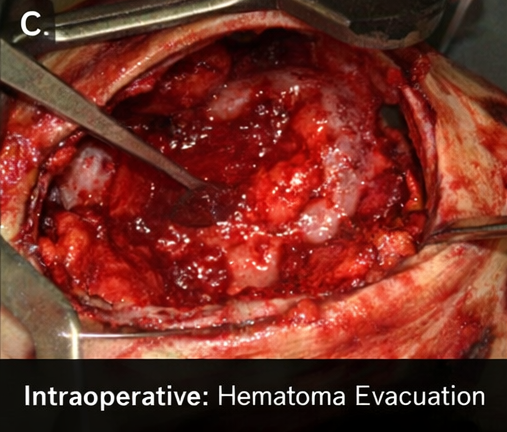
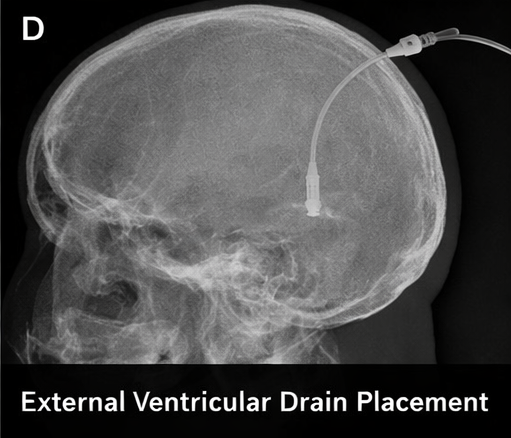
Neurosurgical consultation was obtained urgently. Given the large hematoma volume, mass effect, declining sensorium, and intraventricular extension with early hydrocephalus, the patient underwent decompressive craniectomy with hematoma evacuation.
And placement of an external ventricular drain for cerebrospinal fluid diversion and intracranial pressure monitoring.
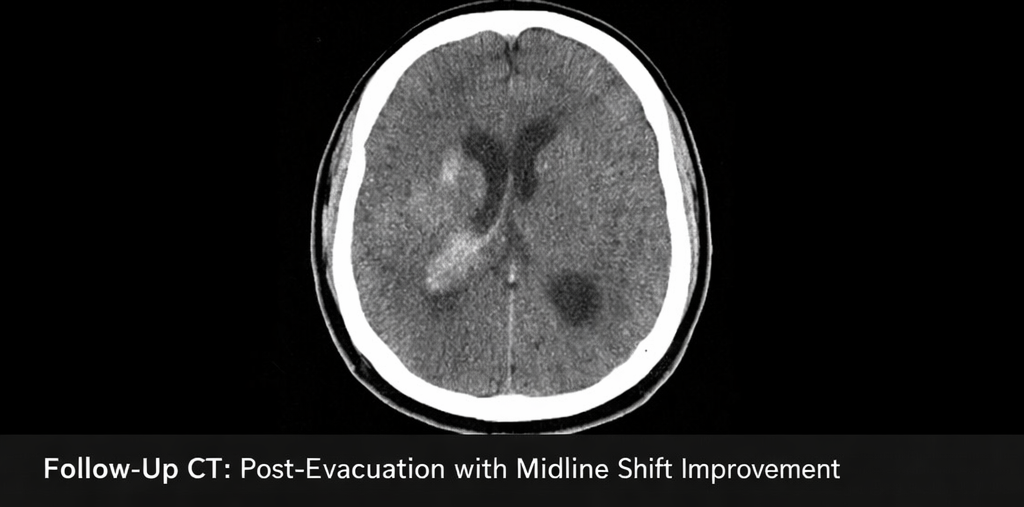
Follow-Up and Outcome
Postoperatively, the patient required mechanical ventilation for 48 hours. Serial CT scans showed satisfactory hematoma evacuation, reduction in midline shift, and improvement in ventricular dilatation. Over the next 10 days, the patient’s level of consciousness improved gradually (GCS 13/15). The external ventricular drain was removed after resolution of hydrocephalus.
At discharge (day 21), the patient had persistent right-sided hemiparesis (power 2/5) and expressive aphasia. He was referred for comprehensive neurorehabilitation, including physiotherapy, speech therapy, and occupational therapy.
At 3-month follow-up, the patient demonstrated partial neurological recovery with improved motor power (3/5) and functional independence in basic activities of daily living with assistance. Blood pressure control was optimized with strict adherence to antihypertensive therapy. No recurrent hemorrhagic events were noted.
Discussion
Large acute intracerebral hemorrhage remains one of the most lethal forms of stroke. Hematoma volume, intraventricular extension, initial GCS, and hematoma expansion are major predictors of mortality and functional outcome. Hypertension is the most common modifiable risk factor, particularly for deep hemorrhages involving the basal ganglia, thalamus, and brainstem.
Non-contrast CT remains the imaging modality of choice for rapid diagnosis, while CT angiography helps exclude secondary causes such as aneurysm or arteriovenous malformation. Acute management focuses on airway protection, hemodynamic stabilization, blood pressure control, management of raised intracranial pressure, and prevention of secondary brain injury.
The role of surgical intervention in ICH remains selective. Hematoma evacuation and decompressive surgery may benefit carefully selected patients with large hematomas, significant mass effect, neurological deterioration, or intraventricular hemorrhage with hydrocephalus. Early multidisciplinary care and structured rehabilitation are critical for improving functional outcomes in survivors.
Conclusion
Large acute intracerebral hemorrhage is a catastrophic neurological emergency requiring rapid diagnosis, aggressive medical stabilization, and timely neurosurgical intervention in selected cases. This case highlights the importance of early neuroimaging, strict blood pressure control, management of raised intracranial pressure, and individualized surgical decision-making. Long-term neurological recovery depends on early critical care, prevention of secondary injury, and comprehensive rehabilitation. Optimizing control of modifiable risk factors such as hypertension remains central to preventing recurrence and improving long-term outcomes.
References
- Qureshi AI, Mendelow AD, Hanley DF. Intracerebral haemorrhage. Lancet. 2009;373(9675):1632–1644.
- Hemphill JC, Greenberg SM, Anderson CS, et al. Guidelines for the management of spontaneous intracerebral hemorrhage. Stroke. 2015;46(7):2032–2060.
- Steiner T, Salman RA-S, Beer R, et al. European Stroke Organisation (ESO) guidelines for the management of spontaneous intracerebral hemorrhage. Int J Stroke. 2014;9(7):840–855.
- Broderick JP, Brott T, Duldner JE, et al. Volume of intracerebral hemorrhage: A powerful and easy-to-use predictor of 30-day mortality. Stroke. 1993;24(7):987–993.
- Morgenstern LB, Frankowski RF, Shedden P, et al. Surgical treatment for intracerebral hemorrhage (STICH): A randomized trial. Lancet. 2005;365(9457):387–397.
- Anderson CS, Heeley E, Huang Y, et al. Rapid blood-pressure lowering in patients with acute intracerebral hemorrhage. N Engl J Med. 2013;368(25):2355–2365.
- Rincon F, Mayer SA. Intracerebral hemorrhage: Clinical overview and pathophysiologic concepts. Transl Stroke Res. 2012;3(Suppl 1):10–24.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
According to the CAPTIVATE Study, fixed-duration ibrutinib plus venetoclax may be beneficial for patients with high-risk chronic lymphocytic leukemia.
2.
Scientists develop novel adjuvant delivery system to enhance cancer vaccine effectiveness
3.
Vepdegestrant Earns FDA Nod for ESR1-Mutated Breast Cancer
4.
According to a study, taking part in a clinical trial for cancer may not actually increase survival.
5.
A new blood test greatly increases the ability to detect cancer.
1.
Cancer Memory: A Persistent Threat to Tumor Recurrence and Metastasis
2.
Unraveling the Mysteries of Hematocrit: How It Impacts Your Health
3.
The Transformative Power of Genomics in the Diagnosis and Management of Rare Cancers
4.
Omega-3 Fatty Acids as Molecular Adjuvants Against Chemoresistance in Breast Cancer
5.
Surprising Symptoms of Prostate Cancer: What You Need to Know
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Navigating the Complexities of Ph Negative ALL - Part X
2.
Efficient Management of First line ALK-rearranged NSCLC - Part III
3.
What Therapy Would Yield the Best Outcomes In Patients with R/R B-cell ALL?
4.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part IV
5.
Updates on Standard V/S High Risk Myeloma Treatment- The Next Part

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge