Avascular Necrosis of the Head of Femur: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Avascular necrosis (AVN) of the head of femur is a progressive orthopedic condition characterized by compromised blood supply to the femoral head, leading to bone ischemia, structural collapse, and secondary osteoarthritis if untreated. It commonly affects young and middle-aged adults and is associated with risk factors such as corticosteroid use, alcohol abuse, trauma, and certain systemic diseases. Clinical presentation ranges from asymptomatic early disease to severe hip pain and functional limitation in advanced stages. Diagnosis relies on clinical suspicion supported by imaging, with magnetic resonance imaging (MRI) being the gold standard for early detection. Management strategies depend on disease stage and include conservative measures, pharmacologic therapy, joint-preserving surgical procedures, and total hip arthroplasty in advanced cases. This case report describes a young patient with avascular necrosis of the femoral head, highlighting clinical features, diagnostic evaluation, management, and short-term outcomes. Early diagnosis and timely intervention are essential to delay disease progression and preserve joint function.
Introduction
Avascular necrosis of the femoral head is a debilitating condition resulting from interruption of the blood supply to the subchondral bone, leading to osteocyte death and eventual collapse of the femoral head. The condition predominantly affects individuals between 20 and 50 years of age and has significant socioeconomic implications due to functional disability.
Common etiological factors include prolonged corticosteroid therapy, excessive alcohol consumption, trauma, hematological disorders, autoimmune diseases, and idiopathic causes. Early stages may be clinically silent, making diagnosis challenging. However, progression of the disease leads to persistent hip pain, reduced range of motion, and impaired mobility. Advances in imaging and surgical techniques have improved early detection and outcomes, but delayed diagnosis often necessitates joint replacement. This case report aims to illustrate the clinical course, diagnostic approach, and management of avascular necrosis of the femoral head in a pediatric patient.
Case Report
Patient History
A 14-year-old male presented to the orthopedic outpatient clinic with a history of progressive left hip pain for three months. The pain was insidious in onset, dull in character, localized to the groin region, and exacerbated by weight-bearing and physical activity. The patient reported difficulty in walking long distances and occasional limping.
There was no history of trauma, fever, or infection. Past medical history revealed intermittent corticosteroid use for nephrotic syndrome over the previous two years. There was no history of alcohol consumption, chronic illness, or similar complaints in the family.
Clinical Examination
On examination, the patient had an antalgic gait favoring the left lower limb.

Vital signs were stable. Local examination of the left hip revealed tenderness in the groin region and restriction of internal rotation and abduction.

Flexion was mildly painful at the extremes of motion. No limb length discrepancy was noted. Examination of the contralateral hip and other joints was normal. Neurological and vascular examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
The differential diagnosis for chronic hip pain in an adolescent included:
- Avascular necrosis of the femoral head
- Slipped capital femoral epiphysis
- Transient synovitis
- Septic arthritis
- Juvenile idiopathic arthritis
Investigations
- Laboratory tests: Complete blood count, inflammatory markers, and metabolic profile were within normal limits.
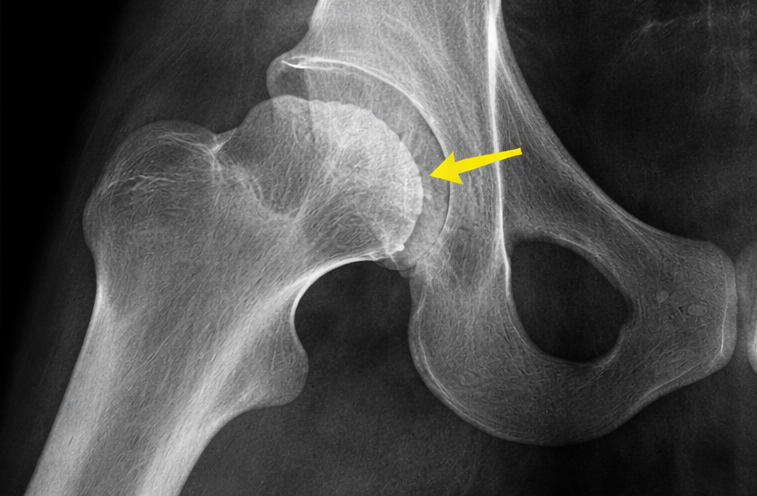
- Plain radiograph (pelvis with both hips): Early flattening and sclerosis of the left femoral head, suggestive of early-stage avascular necrosis.
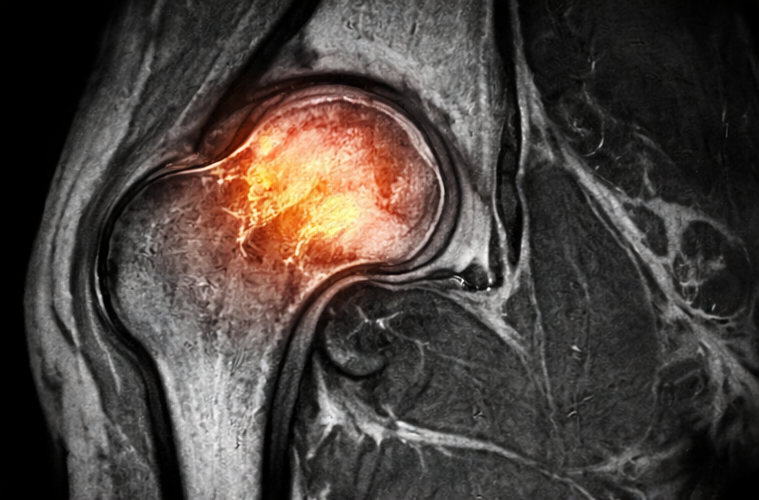
- MRI of the pelvis: Revealed hypointense signals on T1-weighted images and hyperintense signals on T2-weighted images in the left femoral head with bone marrow edema, confirming avascular necrosis (Ficat–Arlet stage II).
- Bone scan: Not performed as MRI findings were diagnostic.
Management and Outcome
Management Strategy
The patient was managed with a joint-preserving approach due to early-stage disease and young age. Management included:
- Activity modification: Restricted weight-bearing on the affected limb using crutches.
- Pharmacologic therapy: Bisphosphonates and analgesics were initiated to reduce bone resorption and manage pain.
- Physiotherapy: Gentle range-of-motion exercises to maintain hip mobility.
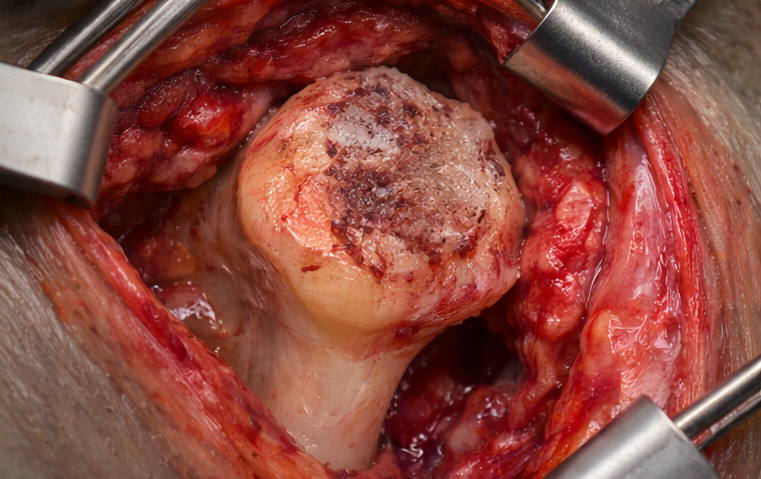
- Surgical intervention: Core decompression of the femoral head was performed to relieve intraosseous pressure and promote revascularization.
- Patient and family education: Counseling regarding disease progression, adherence to treatment, and avoidance of risk factors such as unsupervised steroid use.
Follow-Up and Outcome
At three-month follow-up, the patient reported significant reduction in pain and improvement in gait. Hip range of motion improved, and radiological evaluation showed no progression of femoral head collapse. At six months, the patient was able to resume routine activities with minimal discomfort. Long-term follow-up was planned to monitor disease progression and functional outcomes.
Discussion
Avascular necrosis of the femoral head is a progressive condition that can lead to irreversible joint damage if not identified early. Corticosteroid use is one of the most significant non-traumatic risk factors, particularly in pediatric and adolescent populations with chronic systemic illnesses. The pathogenesis involves lipid metabolism alterations, increased intraosseous pressure, and microvascular compromise.
MRI is the most sensitive modality for early diagnosis, allowing detection before radiographic changes become evident. Early-stage disease can be managed with conservative and joint-preserving surgical techniques such as core decompression, which aims to restore blood flow and delay disease progression. Advanced stages often require total hip arthroplasty, which is less desirable in young patients due to implant longevity concerns.
Multidisciplinary management, early intervention, and patient education are critical to improving outcomes. Regular follow-up is essential to detect progression and guide timely escalation of treatment.
Conclusion
Avascular necrosis of the head of femur is a serious orthopedic condition with the potential for significant morbidity, particularly in young patients. Early recognition through careful clinical assessment and prompt imaging with MRI enables timely intervention and joint preservation. Identification and modification of risk factors, appropriate pharmacologic therapy, and surgical management tailored to disease stage are essential for optimal outcomes. A multidisciplinary approach, combined with patient and family education, plays a pivotal role in preventing disease progression and maintaining long-term hip function. With early diagnosis and appropriate treatment, patients can achieve pain relief, functional improvement, and delayed need for joint replacement.
References
-
Parfitt, A. M. (1994). Osteonecrosis: Pathogenesis and classification. Clinical Orthopaedics and Related Research, 292, 10–21. https://journals.lww.com/clinorthop/Abstract/1994/01000/Osteonecrosis__Pathogenesis_and_Classification.3.aspx
- Mont, M. A., & Hungerford, D. S. (1995). Non-traumatic avascular necrosis of the femoral head. Journal of Bone and Joint Surgery, 77(3), 459–474. https://journals.lww.com/jbjsjournal/Abstract/1995/03000/Nontraumatic_Avascular_Necrosis_of_the.18.aspx
- Assouline-Dayan, Y., Chang, C., Greenspan, A., Shoenfeld, Y., & Gershwin, M. E. (2002). Pathogenesis and natural history of osteonecrosis. Seminars in Arthritis and Rheumatism, 32(2), 94–124. https://doi.org/10.1053/sarh.2002.33724
- Ficat, R. P. (1985). Idiopathic bone necrosis of the femoral head: Early diagnosis and treatment. Journal of Bone and Joint Surgery, 67(1), 3–9.
- https://journals.lww.com/jbjsjournal/Abstract/1985/67010/Idiopathic_Bone_Necrosis_of_the_Femoral.2.aspx
- Hernigou, P., Beaujean, F., & Lambotte, J. C. (1999). Decrease in the mesenchymal stem-cell pool in the proximal femur in corticosteroid-induced osteonecrosis. Journal of Bone and Joint Surgery, 81(3), 349–355. https://journals.lww.com/jbjsjournal/Abstract/1999/03000/Decrease_in_the_Mesenchymal_Stem_Cell.7.aspx
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
According to the CAPTIVATE Study, fixed-duration ibrutinib plus venetoclax may be beneficial for patients with high-risk chronic lymphocytic leukemia.
2.
Scientists develop novel adjuvant delivery system to enhance cancer vaccine effectiveness
3.
Vepdegestrant Earns FDA Nod for ESR1-Mutated Breast Cancer
4.
According to a study, taking part in a clinical trial for cancer may not actually increase survival.
5.
A new blood test greatly increases the ability to detect cancer.
1.
Cancer Memory: A Persistent Threat to Tumor Recurrence and Metastasis
2.
Unraveling the Mysteries of Hematocrit: How It Impacts Your Health
3.
The Transformative Power of Genomics in the Diagnosis and Management of Rare Cancers
4.
Omega-3 Fatty Acids as Molecular Adjuvants Against Chemoresistance in Breast Cancer
5.
Surprising Symptoms of Prostate Cancer: What You Need to Know
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Navigating the Complexities of Ph Negative ALL - Part X
2.
Efficient Management of First line ALK-rearranged NSCLC - Part III
3.
What Therapy Would Yield the Best Outcomes In Patients with R/R B-cell ALL?
4.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part IV
5.
Updates on Standard V/S High Risk Myeloma Treatment- The Next Part

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge