Ocular Melanoma: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Ocular Melanoma is the most common primary intraocular malignancy in adults, arising from melanocytes of the uveal tract, including the iris, ciliary body, and choroid. It is a rare but potentially life-threatening condition due to its high propensity for hematogenous metastasis, particularly to the liver. Early diagnosis remains challenging as initial symptoms may be subtle or absent, leading to delayed presentation.
We report the case of a 55-year-old male presenting with progressive, painless diminution of vision and photopsia. Detailed ophthalmic evaluation and multimodal imaging revealed a pigmented choroidal mass with associated subretinal fluid, consistent with uveal melanoma. The patient was treated with plaque brachytherapy, resulting in tumor regression and stabilization of vision.
This case highlights the importance of early clinical suspicion, appropriate imaging modalities, and multidisciplinary management to optimize outcomes and reduce metastatic risk in patients with ocular melanoma.
Introduction
Uveal Melanoma represents the most common primary intraocular malignancy in adults, with an incidence of approximately 5–7 cases per million per year. The majority of tumors arise from the choroid (~85–90%), followed by the ciliary body and iris. Despite its rarity, uveal melanoma accounts for significant morbidity and mortality due to its aggressive metastatic potential.
The pathogenesis involves malignant transformation of melanocytes, often associated with mutations in GNAQ, GNA11, BAP1, and SF3B1 genes. Tumor growth leads to progressive disruption of retinal architecture and may result in exudative retinal detachment.
Key risk factors include:
• Light iris color and fair skin
• Chronic ultraviolet exposure
• Ocular or oculodermal melanocytosis
• Dysplastic nevus syndrome
• Genetic predisposition
Clinically, patients may present with:
• Blurred or distorted vision
• Photopsia (flashes of light)
• Floaters
• Visual field defects
• Metamorphopsia
• Asymptomatic lesions detected incidentally
Due to the insidious onset and nonspecific symptoms, early diagnosis is often difficult. Delayed detection increases the risk of metastatic dissemination, particularly via hematogenous routes to the liver.
Case Report
Patient History
A 55-year-old male presented to the ophthalmology clinic with:
• Gradual, painless diminution of vision in the right eye for 3 months
• Intermittent flashes of light (photopsia)
• Progressive peripheral visual field loss
There was no history of ocular trauma, surgery, or inflammatory eye disease. The patient had no known systemic comorbidities such as hypertension or diabetes mellitus. There was no family history of ocular malignancy or melanoma.
Clinical Examination
On examination:
• Best-corrected visual acuity: 6/18 (right eye), 6/6 (left eye)
• Intraocular pressure: within normal limits
• Anterior segment: unremarkable
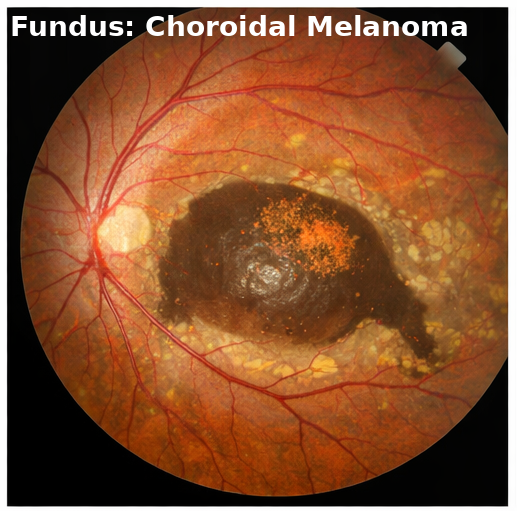
Fundoscopic examination of the right eye revealed:
• A dome-shaped, elevated pigmented lesion in the choroid
• Presence of overlying subretinal fluid
• Areas of orange pigment deposition (lipofuscin)
The left eye examination was normal.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Choroidal melanoma
• Choroidal nevus
• Metastatic intraocular tumor
• Circumscribed choroidal hemangioma
The presence of subretinal fluid, orange pigment, and progressive visual symptoms strongly suggested malignant transformation rather than a benign lesion.
Investigations
Ophthalmic Imaging
• Fundus photography: confirmed pigmented elevated lesion
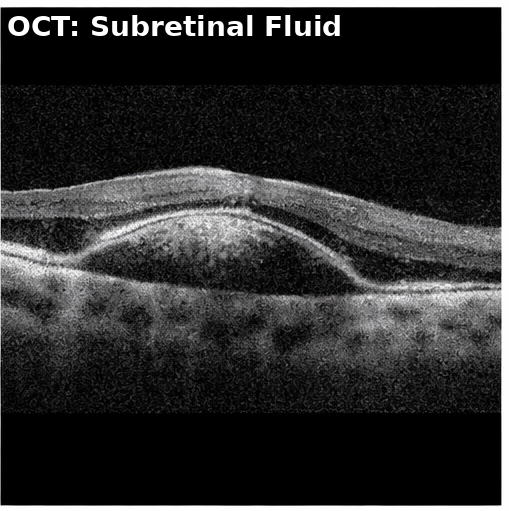
• Optical Coherence Tomography: demonstrated subretinal fluid and neurosensory retinal detachment
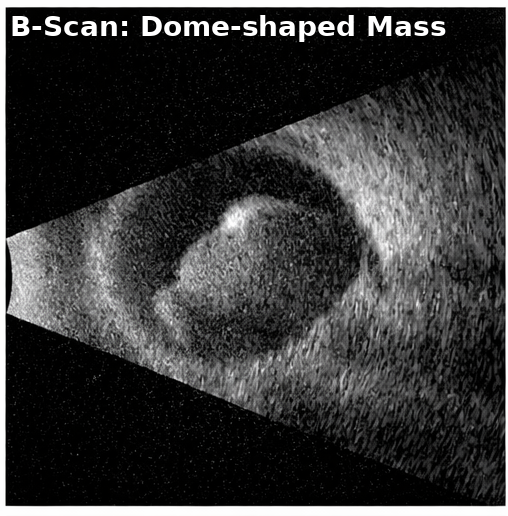
• B-scan Ultrasonography: revealed a dome-shaped mass with low-to-medium internal reflectivity and acoustic hollowness
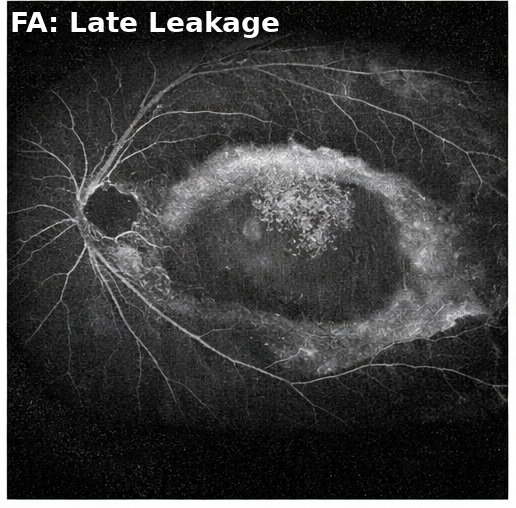
• Fluorescein Angiography: showed early hypofluorescence with late leakage
Tumor dimensions measured approximately 8 mm in basal diameter and 4 mm in thickness.
Systemic Evaluation
• Liver function tests: within normal limits
• Abdominal ultrasound: no evidence of hepatic metastasis
• Chest imaging: unremarkable
Diagnosis
Based on clinical findings and imaging characteristics, a diagnosis of choroidal melanoma was established.
Management and Outcome
Management Strategy
A multidisciplinary approach involving ophthalmology, radiation oncology, and medical oncology teams was adopted.
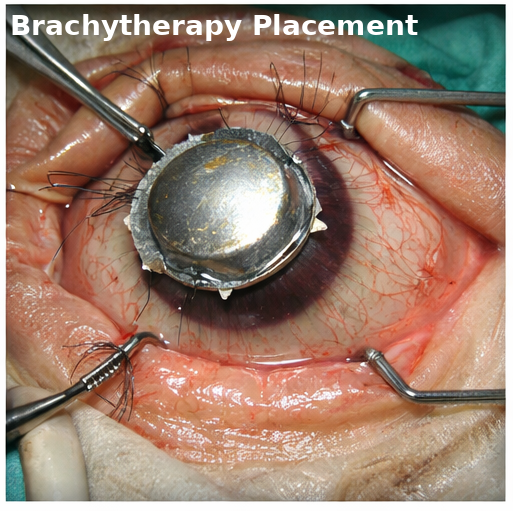
Primary Treatment
• Plaque brachytherapy using Brachytherapy (Iodine-125)
Supportive Management
• Regular ophthalmic monitoring
• Patient counseling regarding visual prognosis
• Surveillance for metastatic disease
Follow-Up and Outcome
At 3 months:
• Reduction in tumor thickness
• Stabilization of visual acuity
At 6 months:
• Resolution of subretinal fluid
• No evidence of tumor progression
At 12 months:
• Significant tumor regression
• No signs of systemic metastasis
• Improved quality of life
Discussion
Pathophysiology
Ocular melanoma arises from uncontrolled proliferation of melanocytes within the uveal tract. Progressive tumor growth leads to:
• Mechanical disruption of retinal layers
• Exudation causing subretinal fluid accumulation
• Increased intraocular pressure in advanced cases
Metastasis occurs predominantly via hematogenous spread, with the liver being the most common site due to its vascular nature.
Diagnostic Challenges
Early diagnosis can be difficult due to:
• Asymptomatic early stages
• Similar appearance to benign choroidal nevi
• Lack of routine screening
Key diagnostic modalities include:
• Fundoscopy
• Ultrasonography (gold standard for intraocular tumors)
• OCT for retinal involvement
• Angiography for vascular patterns
Treatment Considerations
Radiation Therapy
• Brachytherapy remains the standard of care for small to medium tumors
• Provides local tumor control with globe preservation
Surgical Management
• Enucleation is considered for large tumors or those with severe complications
Systemic Therapy
• Immunotherapy and targeted therapy are used in metastatic disease
Complications
Potential complications include:
• Vision loss
• Radiation retinopathy
• Optic neuropathy
• Secondary glaucoma
• Metastatic spread (especially liver)
Prognosis
Prognosis depends on:
• Tumor size and thickness
• Location within the eye
• Genetic mutations (e.g., BAP1)
• Presence of metastasis
Five-year survival rates vary, with localized disease having a relatively favorable prognosis, while metastatic disease significantly reduces survival outcomes.
Conclusion
Ocular melanoma is a rare yet aggressive intraocular malignancy requiring early detection and prompt intervention. This case highlights the importance of recognizing early visual symptoms such as blurred vision and photopsia.
Imaging plays a crucial role in diagnosis, with ultrasonography and OCT providing valuable structural insights. Management requires a comprehensive, multidisciplinary approach involving radiation therapy, regular follow-up, and systemic surveillance.
Strict monitoring for metastatic disease, especially hepatic involvement, is essential in long-term care. Early diagnosis and appropriate treatment can significantly improve visual outcomes and overall survival in patients with ocular melanoma.
References
- Singh AD, Turell ME, Topham AK. Uveal melanoma: trends in incidence, treatment, and survival. Ophthalmology. https://pubmed.ncbi.nlm.nih.gov/18061270/
- Kujala E, Mäkitie T, Kivelä T. Very long-term prognosis of patients with malignant uveal melanoma. Invest Ophthalmol Vis Sci. https://pubmed.ncbi.nlm.nih.gov/17460265/
- Shields CL, Kaliki S, Furuta M, et al. Clinical spectrum and prognosis of uveal melanoma. Retina. https://pubmed.ncbi.nlm.nih.gov/23760462/
- Damato B, Dukes J, Goodall H, Carvajal RD. Tebentafusp: T-cell redirection therapy in uveal melanoma. Lancet Oncol. https://pubmed.ncbi.nlm.nih.gov/33539743/
- Collaborative Ocular Melanoma Study Group. The COMS randomized trial of iodine 125 brachytherapy. Arch Ophthalmol. https://pubmed.ncbi.nlm.nih.gov/9659486/
- Jager MJ, Shields CL, Cebulla CM, et al. Uveal melanoma. Nat Rev Dis Primers. https://pubmed.ncbi.nlm.nih.gov/28655880/
- Finger PT. Radiation therapy for choroidal melanoma. Surv Ophthalmol. https://pubmed.ncbi.nlm.nih.gov/20399433/
- Carvajal RD, Schwartz GK, Tezel T, et al. Metastatic disease from uveal melanoma. Cancer. https://pubmed.ncbi.nlm.nih.gov/20672353/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge