Esophageal Candidiasis: Clinical Presentation, Diagnostic Evaluation, and Management - A Case Report
OthersPage Navigation
Abstract
Esophageal candidiasis is an opportunistic fungal infection of the esophagus most commonly caused by Candida albicans. It predominantly affects individuals with impaired immunity, including those with diabetes mellitus, human immunodeficiency virus (HIV) infection, malignancy, or prolonged exposure to antibiotics or corticosteroids. Clinically, it presents with dysphagia, odynophagia, retrosternal pain, and reduced oral intake, leading to significant morbidity if left untreated.
We report a case of esophageal candidiasis in a middle-aged patient with poorly controlled diabetes mellitus, presenting with progressive dysphagia and odynophagia. This case highlights the clinical features, diagnostic challenges, endoscopic findings, therapeutic management, and outcome. The report emphasizes the importance of early recognition, risk factor identification, and timely antifungal therapy to achieve favorable clinical outcomes and prevent complications.
Introduction
Esophageal candidiasis is the most common cause of infectious esophagitis worldwide and represents a frequent manifestation of opportunistic fungal infections. Although Candida species are normal commensals of the gastrointestinal tract, disruption of host defense mechanisms can lead to pathological overgrowth and mucosal invasion. The condition is particularly prevalent among immunocompromised individuals, including patients with HIV/AIDS, diabetes mellitus, hematological malignancies, organ transplant recipients, and those receiving immunosuppressive therapies.
The disease can also occur in immunocompetent individuals, especially in the presence of predisposing factors such as prolonged antibiotic use, proton pump inhibitor therapy, or esophageal motility disorders. Clinically, esophageal candidiasis presents with non-specific symptoms that may overlap with gastroesophageal reflux disease, pill-induced esophagitis, or malignancy, often leading to delayed diagnosis.
Endoscopic evaluation remains the cornerstone of diagnosis, with characteristic white plaques adherent to the esophageal mucosa. Histopathological and microbiological confirmation is useful in atypical or refractory cases. This case report aims to describe a classical presentation of esophageal candidiasis, outline diagnostic considerations, and discuss evidence-based management strategies.
Case Report
Patient History
A 45-year-old man presented to the gastroenterology outpatient department with a 3-week history of progressively worsening dysphagia. Initially, the difficulty was limited to solid foods but later progressed to include liquids. The patient also complained of painful swallowing (odynophagia) and a persistent retrosternal burning sensation.
He reported unintentional weight loss of approximately 4 kg over one month, attributed to reduced oral intake due to discomfort. The patient had a known history of type 2 diabetes mellitus for the past 8 years, with irregular medication adherence and poor glycemic control. He also reported recent use of broad-spectrum antibiotics for a lower respiratory tract infection two months prior to presentation.
There was no history of smoking, alcohol consumption, corrosive ingestion, or prior esophageal disease. The patient denied hematemesis or melena. Family history was non-contributory.
Clinical Examination
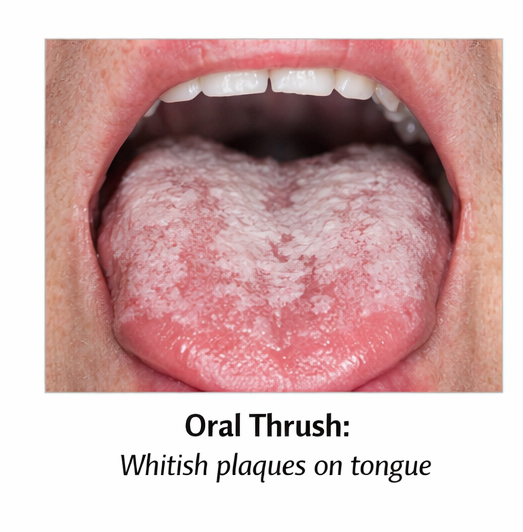
On physical examination, the patient appeared mildly cachectic but was hemodynamically stable. Oral cavity examination revealed whitish, curd-like plaques over the tongue and buccal mucosa that could be scraped off, leaving an erythematous base.
Abdominal examination was normal, with no organomegaly or tenderness. Cardiovascular, respiratory, and neurological examinations were unremarkable. No lymphadenopathy or cutaneous lesions were noted.
Clinical Evaluation
Differential Diagnosis
Based on the presenting symptoms and clinical findings, the following differential diagnoses were considered:
• Esophageal candidiasis
• Viral esophagitis (herpes simplex virus or cytomegalovirus)
• Gastroesophageal reflux disease
• Pill-induced esophagitis
• Esophageal malignancy
The presence of oral candidiasis, metabolic risk factors, and predominant odynophagia favored a diagnosis of infectious esophagitis, particularly esophageal candidiasis.
Investigations
Laboratory Studies
Baseline laboratory investigations showed elevated fasting plasma glucose levels and an HbA1c of 9.2%, indicating poor glycemic control. Complete blood count, liver function tests, and renal function parameters were within normal limits. HIV serology was negative.
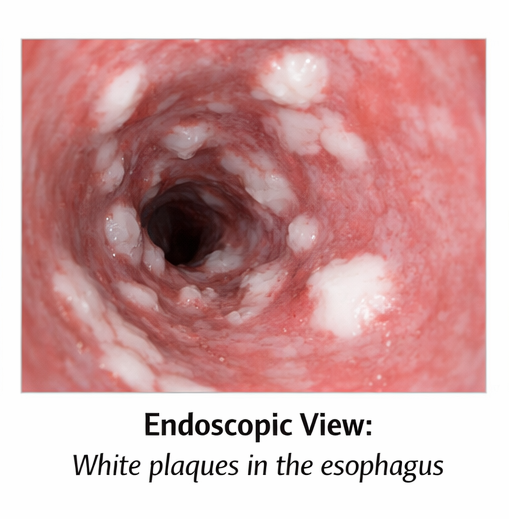
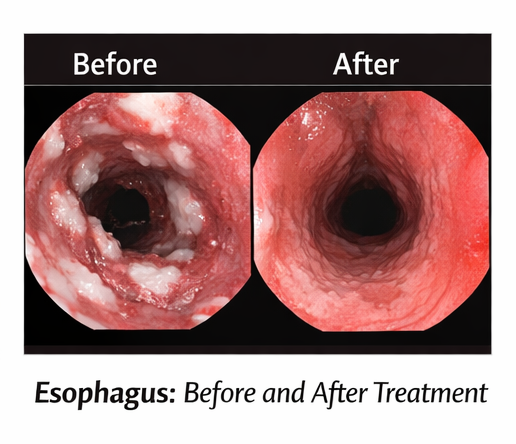
Upper gastrointestinal endoscopy revealed multiple discrete and confluent white plaques adherent to the esophageal mucosa, predominantly involving the mid and distal esophagus. The underlying mucosa appeared erythematous and friable, with focal erosions. There was no evidence of strictures or mass lesions.
Microbiological and Histopathological Evaluation
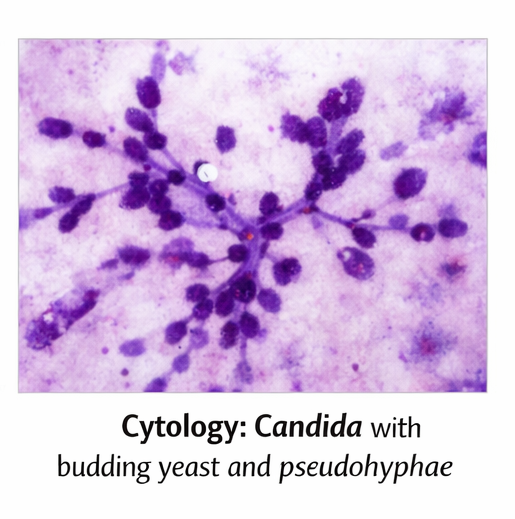
Brush cytology and biopsy specimens obtained during endoscopy demonstrated budding yeast forms and pseudohyphae on potassium hydroxide preparation and periodic acid–Schiff staining, consistent with Candida species. No viral inclusion bodies or malignant cells were identified.
Diagnosis
A definitive diagnosis of esophageal candidiasis was established based on characteristic endoscopic findings and microbiological confirmation in the presence of known predisposing risk factors.
Management and Outcome
Therapeutic Management
The patient was initiated on systemic antifungal therapy with oral fluconazole, given as a 200 mg loading dose followed by 100 mg once daily for 14 days.

Supportive management included dietary modification with soft, non-irritating foods, adequate hydration, and analgesics as required. Optimization of glycemic control was addressed through adjustment of antidiabetic medications and dietary counseling.
The patient was educated regarding the importance of medication adherence and risk factor modification to prevent recurrence.
Outcome
The patient reported significant improvement in odynophagia and dysphagia within 5–7 days of starting antifungal therapy. At the completion of the 14-day course, symptoms had completely resolved, and oral lesions had disappeared.
At 3-month follow-up, the patient remained asymptomatic, had regained weight, and demonstrated improved glycemic control. No recurrence was reported.
Discussion
Esophageal candidiasis is a common opportunistic infection with a well-established association with immunosuppression and metabolic disorders. Diabetes mellitus contributes to susceptibility by impairing neutrophil function and altering mucosal immunity, thereby facilitating fungal overgrowth.
Clinically, esophageal candidiasis is characterized by dysphagia and odynophagia, although asymptomatic cases may occur. Endoscopy typically reveals white plaques that are adherent and difficult to wash off, distinguishing them from food residue.
Differentiation from viral esophagitis is crucial, as herpes simplex virus commonly causes discrete ulcers, while cytomegalovirus presents with large, linear ulcers. Fluconazole remains the first-line therapy due to its high efficacy, favorable safety profile, and excellent esophageal penetration.
Addressing underlying risk factors, such as uncontrolled diabetes or inappropriate antibiotic use, is essential to prevent recurrence. This case highlights the importance of a comprehensive, multidisciplinary approach in managing esophageal candidiasis.
Conclusion
Esophageal candidiasis should be suspected in patients presenting with dysphagia or odynophagia, particularly in the presence of immunosuppressive or metabolic risk factors. Prompt endoscopic evaluation and early initiation of antifungal therapy result in rapid symptom resolution and favorable outcomes. Long-term management should focus on correction of underlying predisposing factors to reduce recurrence and disease burden.
References
- Wilcox CM. Esophageal infections: etiology, diagnosis, and management. Gastroenterol Clin North Am. 1996;25(3):689–706.
- Kliemann DA, et al. Candida esophagitis: species distribution and risk factors. Mycoses. 2008;51(6):488–494.
- Kodsi BE, et al. Candida esophagitis: a prospective study of 27 cases. Gastroenterology. 1976;71(5):715–719.
- Pappas PG, et al. Clinical practice guideline for the management of candidiasis. Clin Infect Dis. 2016;62(4):e1–e50.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Newly identified T-cell subtype may explain treatment-resistant childhood leukemia
2.
Glioblastoma treatment breakthrough shows promise
3.
A computer-aided diagnostic system for improved detection of breast cancer.
4.
Patients With Melanoma Brain Mets May Fare Better With RT Before Immunotherapy
5.
Browse the NBE-Released Curriculum at FNB Head and Neck Oncology.
1.
Liquid Biopsies in Hematology: A Window into the Disease
2.
Unleashing the Power of AI: A Systematic Review of Predictive Biomarker Discovery in Immuno-Oncology
3.
A Visual Guide to Understanding Breast Cancer Staging
4.
Exploring the Latest Treatments for Essential Thrombocythemia
5.
Innovative Marketing Strategies for Oncology Drugs: A Clinician’s Take on Digital and B2B Trends
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part III
2.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part V
3.
An Intro to The Multifaceted Advantages of CDK4/6 Inhibitors in HR+/HER2- Advanced Breast Cancer Clinical Studies.
4.
Current Scenario of Cancer- An Overview of The Incidence of Cancer in Men
5.
Navigating the Complexities of Ph Negative ALL - Part II

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge