Nephrotic Syndrome Presenting with Generalized Edema and Heavy Proteinuria in a Young Adult: A Case Report
OthersPage Navigation
Abstract
Nephrotic syndrome is a clinical condition characterized by massive proteinuria, hypoalbuminemia, generalized edema, and hyperlipidemia resulting from increased glomerular permeability. It may arise from primary glomerular diseases or secondary systemic disorders such as diabetes mellitus, systemic lupus erythematosus, infections, and malignancies. Early diagnosis through clinical assessment, laboratory investigations, renal imaging, and histopathological evaluation is essential to prevent complications including thromboembolism, infections, acute kidney injury, and chronic kidney disease. We report the case of a 27-year-old man who presented with progressive bilateral lower-limb swelling, facial puffiness, and frothy urine for three weeks. Laboratory investigations revealed nephrotic-range proteinuria, severe hypoalbuminemia, hypercholesterolemia, and preserved renal function. Renal biopsy demonstrated minimal change disease. The patient was treated with corticosteroids, angiotensin-converting enzyme inhibitor therapy, diuretics, dietary salt restriction, and supportive care. Significant clinical and biochemical improvement was observed over six months of follow-up. This case emphasizes the importance of prompt recognition, appropriate diagnostic evaluation, and individualized treatment in achieving remission and preventing disease-related complications.
Introduction
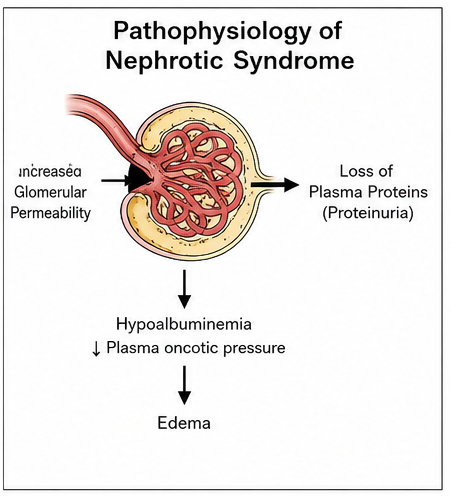
Nephrotic syndrome is one of the most common manifestations of glomerular disease and is defined by proteinuria exceeding 3.5 g/day, hypoalbuminemia, generalized edema, and hyperlipidemia. Damage to the glomerular filtration barrier permits excessive urinary loss of plasma proteins, particularly albumin, resulting in decreased plasma oncotic pressure and subsequent fluid accumulation within interstitial tissues.
The syndrome may result from primary glomerular disorders such as minimal change disease, focal segmental glomerulosclerosis, and membranous nephropathy or secondary conditions including diabetes mellitus, systemic lupus erythematosus, amyloidosis, viral infections, medications, and malignancies. Minimal change disease remains the predominant cause in children, whereas membranous nephropathy and focal segmental glomerulosclerosis are increasingly recognized among adults.
Patients commonly present with peripheral edema, facial puffiness, ascites, weight gain, frothy urine, fatigue, and reduced exercise tolerance. Delayed diagnosis may lead to severe infections, venous thromboembolism, progressive renal dysfunction, and cardiovascular complications. Early diagnosis and appropriate therapy significantly improve clinical outcomes and preserve renal function.
Case Report
A 27-year-old man presented to the nephrology outpatient department with progressive swelling of both legs and puffiness around the eyes for three weeks. He also reported frothy urine, increasing abdominal fullness, and a weight gain of nearly 6 kg during the previous month. He denied fever, dysuria, hematuria, joint pain, skin rash, or recent upper respiratory tract infection.

His medical history was unremarkable, with no known diabetes, hypertension, autoimmune disease, or chronic kidney disease. There was no family history of renal disorders, and he was not taking any nephrotoxic medications.
On examination, the patient appeared comfortable but had marked bilateral pitting pedal edema

extending up to the knees and significant periorbital edema.
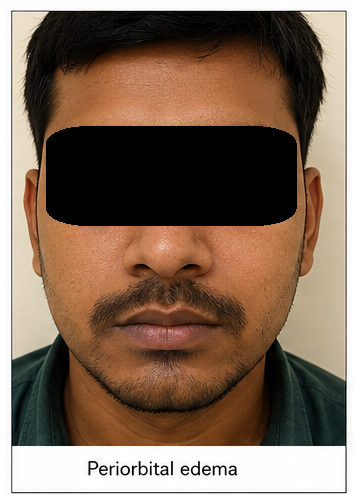
His blood pressure was 128/78 mmHg, pulse rate was 82 beats/minute, respiratory rate was 18 breaths/minute, and oxygen saturation was 98% on room air. Mild abdominal distension with shifting dullness suggested minimal ascites. Cardiovascular, respiratory, and neurological examinations were otherwise unremarkable.
Laboratory investigations demonstrated serum albumin of 2.1 g/dL, total protein of 5.0 g/dL, serum creatinine of 0.9 mg/dL, blood urea nitrogen of 18 mg/dL, total cholesterol of 342 mg/dL, LDL cholesterol of 228 mg/dL, and triglycerides of 276 mg/dL. Urinalysis revealed 4+ proteinuria without hematuria, while 24-hour urinary protein excretion measured 6.8 g/day. Urine microscopy showed occasional hyaline casts without red blood cell casts.
Autoimmune evaluation including antinuclear antibody, anti-double stranded DNA antibody, complement levels, hepatitis B surface antigen, hepatitis C antibody, and HIV serology was negative. Renal ultrasonography demonstrated kidneys of normal size with preserved corticomedullary differentiation and no evidence of obstruction.
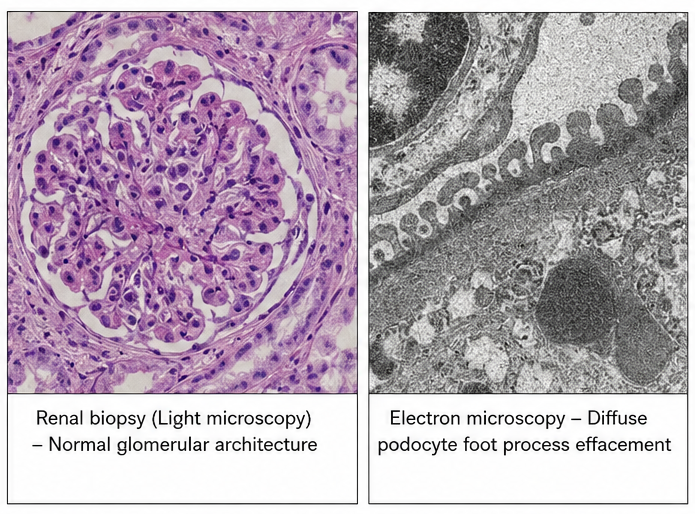
Percutaneous renal biopsy was performed to establish the underlying etiology. Light microscopy revealed normal glomerular architecture without proliferative changes, while electron microscopy demonstrated diffuse podocyte foot process effacement, consistent with minimal change disease.
Based on the clinical presentation, laboratory findings, and histopathological evaluation, a diagnosis of primary nephrotic syndrome secondary to minimal change disease was established.
Management and Outcome
The patient was admitted for initiation of treatment and monitoring of fluid status. Oral prednisolone was started at a dose of 1 mg/kg/day as first-line therapy. An angiotensin-converting enzyme inhibitor was initiated to reduce intraglomerular pressure and decrease urinary protein excretion. Loop diuretics were administered to relieve edema while maintaining careful electrolyte balance.
Dietary counseling emphasized sodium restriction, moderate protein intake, avoidance of excessive fluid consumption, and regular monitoring of body weight. Statin therapy was initiated to address marked hyperlipidemia. Calcium and vitamin D supplementation were prescribed because of prolonged corticosteroid therapy.
The patient tolerated treatment well without infectious or metabolic complications. Progressive reduction in edema was observed during hospitalization, allowing discharge with close outpatient follow-up.
Follow-up
One Month
- Marked reduction in pedal edema and facial swelling.
- Body weight decreased by approximately 4 kg.
- Serum albumin improved to 2.9 g/dL.
- Twenty-four-hour urinary protein declined to 2.8 g/day.
Three Months
- Complete resolution of generalized edema.
- Serum albumin increased to 3.8 g/dL.
- Urinary protein excretion decreased to less than 500 mg/day.
- Lipid profile demonstrated significant improvement.
- Serum creatinine remained within the normal range.
Six Months
The patient achieved complete clinical and biochemical remission. Repeat urine protein estimation showed minimal residual proteinuria, serum albumin normalized to 4.2 g/dL, and cholesterol levels returned near normal. Corticosteroids were gradually tapered according to standard treatment protocols. The patient resumed normal daily activities without recurrence of edema and continued regular nephrology follow-up.
Discussion
Nephrotic syndrome represents a clinical consequence of increased permeability of the glomerular filtration barrier caused by injury to podocytes and the glomerular basement membrane. Massive urinary protein loss results in hypoalbuminemia, decreased plasma oncotic pressure, sodium retention, and generalized edema. Compensatory hepatic lipoprotein synthesis contributes to hyperlipidemia, while urinary loss of anticoagulant proteins increases the risk of venous thromboembolism.
The diagnostic approach requires confirmation of nephrotic-range proteinuria, assessment of renal function, identification of secondary causes, and renal biopsy in selected adult patients. Urinary protein quantification, serum albumin measurement, lipid profile, renal function tests, immunological investigations, and renal imaging constitute the cornerstone of evaluation.
Minimal change disease accounts for approximately 10–15% of nephrotic syndrome cases in adults and is characterized by diffuse podocyte foot process effacement visible only on electron microscopy. The majority of patients respond favorably to corticosteroid therapy, although relapses may occur and require prolonged immunosuppressive management.
Supportive treatment plays an equally important role alongside immunosuppressive therapy. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers reduce proteinuria and delay progression of renal disease. Diuretics effectively control edema, while statins improve dyslipidemia and reduce cardiovascular risk. Vaccination, infection prevention, nutritional counseling, and thromboembolic risk assessment remain essential components of comprehensive patient care.
This case demonstrates that timely diagnosis, exclusion of secondary causes, and prompt initiation of corticosteroid therapy can achieve sustained remission while preserving long-term renal function.
Prognosis
The prognosis of nephrotic syndrome depends on the underlying glomerular disease, response to therapy, frequency of relapse, and development of complications. Patients with minimal change disease generally have an excellent prognosis, with most achieving complete remission following corticosteroid therapy. Long-term monitoring remains necessary to detect relapses, monitor treatment-related adverse effects, assess renal function, and identify progression to chronic kidney disease. Early diagnosis, individualized treatment, and regular follow-up substantially improve renal and cardiovascular outcomes.
Conclusion
Nephrotic syndrome is an important manifestation of glomerular disease that requires early recognition and systematic evaluation to identify its underlying cause. Clinical assessment combined with laboratory investigations, renal imaging, and renal biopsy facilitates accurate diagnosis and guides evidence-based therapy. Corticosteroids remain the cornerstone of treatment for minimal change disease, while supportive measures including renin-angiotensin system blockade, diuretics, lipid-lowering therapy, and dietary modification significantly improve patient outcomes. Regular follow-up is essential for monitoring remission, preventing complications, and preserving long-term renal function.
References
- Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases. Kidney International. 2021;100(4 Suppl):S1–S276. https://pubmed.ncbi.nlm.nih.gov/34556256/
- Rovin BH, Adler SG, Barratt J, et al. Executive summary of the KDIGO 2021 Guideline for the Management of Glomerular Diseases. Kidney International. 2021;100(4):753–779. https://pubmed.ncbi.nlm.nih.gov/34556255/
- Kodner C. Nephrotic syndrome in adults: Diagnosis and management. American Family Physician. 2016;93(6):479–485. https://pubmed.ncbi.nlm.nih.gov/26926897/
- Glassock RJ. The pathogenesis of nephrotic syndrome in minimal change disease. Nephrology Dialysis Transplantation. 2019;34(3):364–366. https://pubmed.ncbi.nlm.nih.gov/30517660/
- Floege J, Amann K. Primary glomerular diseases. The Lancet. 2016;387(10032):2036–2048. https://pubmed.ncbi.nlm.nih.gov/27159779/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
I Was Told I Had 6 Months to Live. That Was 20 Years Ago.
2.
Which Salvage Therapy Is Best for Recurrent Prostate Cancer?
3.
Aspirin Fails to Boost Survival in Colorectal Cancer Trial
4.
Chemoimmunotherapy Boosts Head and Neck Cancer Response
5.
Researchers use AI to monitor side effects of chemotherapy and support families dealing with pediatric cancer.
1.
Essential Developments in Oncology for Healthcare Excellence
2.
Beta-2 Microglobulin: Function, Role in Disease & Clinical Significance Explained
3.
Understanding Apoplexy: Symptoms, Causes, and Treatment Options
4.
Deciphering FFR: A Comprehensive Guide to Understanding Its Meaning
5.
Understanding the Rare Disease: Werner Syndrome Explained
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Should We Use DARA Up Front As First-Line Therapy in MM?
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Current Scenario of Cancer- Palliative Care to Close the Care Gap
4.
What Therapy Would Yield the Best Outcomes In Patients with R/R B-cell ALL?
5.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC: A Continuation

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge