Sigmoid Volvulus: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Sigmoid volvulus is a potentially life-threatening cause of large bowel obstruction characterized by twisting of the sigmoid colon around its mesenteric axis. This torsion leads to luminal obstruction and compromised blood flow, which may progress to bowel ischemia, perforation, and sepsis if untreated. Sigmoid volvulus accounts for a significant proportion of colonic obstructions, particularly in elderly individuals, patients with chronic constipation, and those with redundant sigmoid colon anatomy. Patients typically present with abdominal distension, pain, constipation, and vomiting. Diagnosis relies on clinical suspicion supported by radiological findings such as the classic “coffee bean sign” on abdominal radiographs or confirmatory findings on computed tomography (CT). Prompt intervention is essential, and management may include endoscopic decompression or surgical intervention depending on disease severity and bowel viability. This report describes a case of sigmoid volvulus in an elderly patient who presented with acute intestinal obstruction and was successfully treated with surgical management.
Introduction
Sigmoid volvulus is a condition in which the sigmoid colon twists around its mesenteric attachment, leading to closed-loop intestinal obstruction. It is one of the most common causes of large bowel obstruction worldwide and represents a surgical emergency when associated with ischemia or perforation. The condition is more frequently observed in elderly individuals, particularly in populations with high-fiber diets, chronic constipation, or anatomical predisposition such as an elongated sigmoid colon.
The pathophysiology involves torsion of the sigmoid colon, which results in luminal obstruction and venous congestion. If untreated, this may lead to bowel ischemia, necrosis, and perforation, resulting in peritonitis and septic shock. Risk factors include chronic constipation, neurological disorders, institutionalization, previous abdominal surgery, and megacolon.
Clinical manifestations usually include progressive abdominal distension, abdominal pain, obstipation, and vomiting. Diagnosis is primarily based on imaging studies such as abdominal radiography or CT scan, which demonstrate characteristic findings of volvulus.
Early recognition and timely management are crucial to prevent serious complications. This report describes a case of sigmoid volvulus presenting with acute large bowel obstruction that was diagnosed through imaging and successfully managed with surgical intervention.
Case Report
Patient History
A 68-year-old male presented to the emergency department with complaints of progressive abdominal distension and abdominal pain for two days. The pain was diffuse, colicky in nature, and associated with nausea and repeated episodes of vomiting. The patient also reported inability to pass stool or flatus for the previous 48 hours.
The patient had a history of chronic constipation for several years and required frequent use of laxatives. There was no history of previous abdominal surgery or inflammatory bowel disease. His medical history included hypertension controlled with medication.
Clinical Examination
On physical examination, the patient appeared uncomfortable and mildly dehydrated.
Vital signs:
- Blood pressure: 130/85 mmHg
- Pulse: 96 beats per minute
- Temperature: 37.3°C
- Respiratory rate: 18 breaths per minute
Abdominal examination findings:
- Marked abdominal distension
- Tympanic percussion note
- Mild diffuse tenderness without guarding
- Visible bowel loops
- Absent bowel movements for two days
Digital rectal examination revealed an empty rectum.
Clinical Evaluation
Differential Diagnosis
Based on the presenting symptoms, the following conditions were considered:
- Sigmoid volvulus
- Large bowel obstruction due to colorectal carcinoma
- Fecal impaction
- Pseudo-obstruction (Ogilvie syndrome)
Further imaging studies were performed to confirm the diagnosis.
Investigations
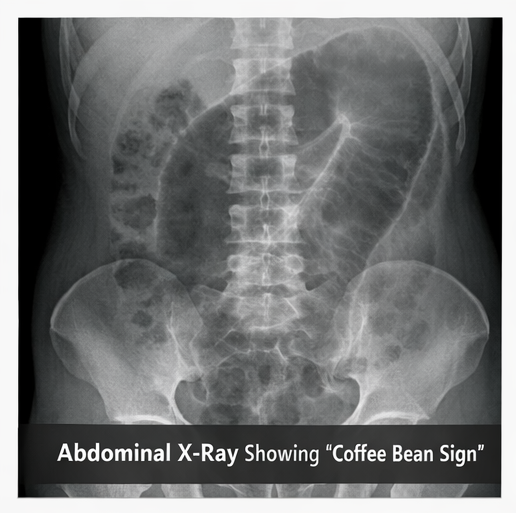
Abdominal Radiography
Plain abdominal X-ray revealed a markedly dilated loop of colon arising from the pelvis with the characteristic “coffee bean” appearance, suggestive of sigmoid volvulus.
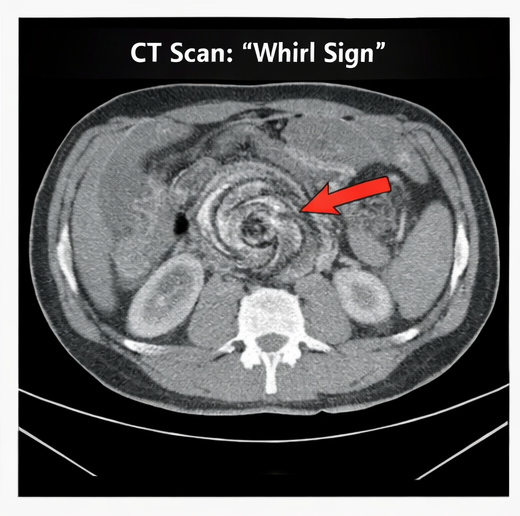
Computed Tomography (CT) Scan
Contrast-enhanced CT scan of the abdomen demonstrated:
- Markedly dilated sigmoid colon
- Twisting of mesenteric vessels producing the “whirl sign”
- Transition point in the sigmoid colon
- No evidence of bowel perforation
These findings confirmed the diagnosis of sigmoid volvulus.
Diagnosis
Based on the clinical findings and imaging results, a diagnosis of acute sigmoid volvulus causing large bowel obstruction was established.
Management and Outcome
Initial Management
The patient was initially stabilized with:
- Intravenous fluid resuscitation
- Nasogastric decompression
- Electrolyte correction
- Broad-spectrum intravenous antibiotics
Endoscopic decompression was considered but deferred due to significant colonic dilation and concern for possible vascular compromise.
Surgical Management
Emergency exploratory laparotomy was performed.
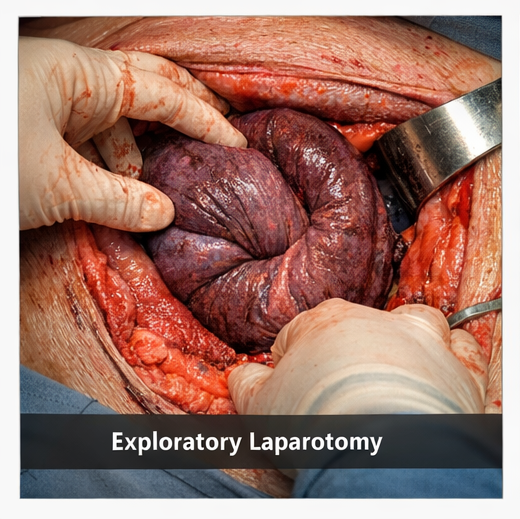
Intraoperative findings:
- A 360-degree torsion of the sigmoid colon around its mesentery
- Markedly dilated sigmoid colon
- No evidence of gangrene or perforation
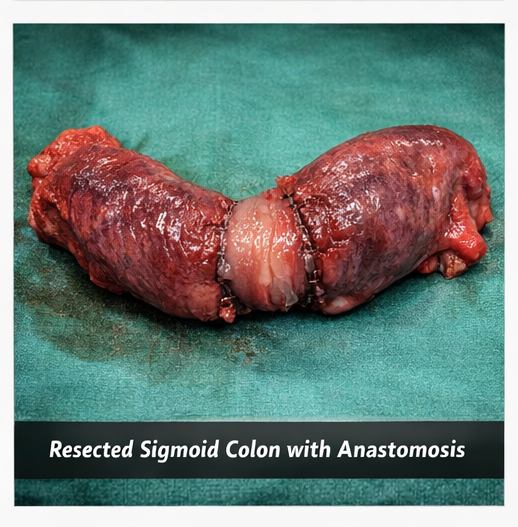
The surgical procedure included:
- Detorsion of the sigmoid colon
- Resection of the redundant sigmoid segment
- Primary colorectal anastomosis
Follow-Up and Outcome
The postoperative course was uneventful.
Postoperative outcomes:
- Gradual resolution of abdominal distension
- Return of bowel function by postoperative day 3
- Tolerance of oral diet by day 5
The patient was discharged on postoperative day 7 in stable condition.
At one-month follow-up:
- The patient remained asymptomatic
- No recurrence of bowel obstruction
- Normal bowel habits were reported
Discussion
Sigmoid volvulus is an important cause of large bowel obstruction and accounts for approximately 8–10% of cases of intestinal obstruction in developed countries. The condition occurs when a redundant sigmoid colon rotates around its mesenteric axis, resulting in obstruction and possible vascular compromise.
Several predisposing factors contribute to the development of sigmoid volvulus, including chronic constipation, advanced age, institutionalization, neurological disorders, and dietary habits that promote colonic elongation.
The classic presentation includes abdominal distension, abdominal pain, constipation, and vomiting. Radiological evaluation plays a critical role in diagnosis. Plain abdominal radiographs often demonstrate the coffee bean sign, while CT imaging provides more detailed visualization, including the whirl sign of twisted mesenteric vessels.
Management depends on the presence of complications such as ischemia or perforation. In stable patients without signs of bowel ischemia, endoscopic detorsion using flexible sigmoidoscopy is often the initial treatment. However, recurrence rates remain high if definitive surgical management is not performed.
Surgical intervention, such as sigmoid resection with primary anastomosis, is recommended in many cases to prevent recurrence and provide definitive treatment.
Early diagnosis and prompt management significantly reduce morbidity and mortality associated with sigmoid volvulus.
Conclusion
Sigmoid volvulus is an important and potentially life-threatening cause of large bowel obstruction that requires prompt recognition and timely management. The condition typically presents with abdominal distension, abdominal pain, constipation, and vomiting, particularly in elderly patients or individuals with chronic constipation and redundant sigmoid colon anatomy. Early clinical suspicion supported by appropriate imaging studies such as abdominal radiography and computed tomography is essential for accurate diagnosis.
Radiological findings including the characteristic coffee bean sign on abdominal X-ray and the whirl sign on CT scan play a crucial role in confirming the diagnosis and guiding treatment decisions. Initial management focuses on patient stabilization through fluid resuscitation, gastrointestinal decompression, and correction of electrolyte imbalances.
Depending on the clinical condition and presence of complications, treatment options include endoscopic decompression or surgical intervention. Definitive surgical procedures such as sigmoid resection with primary anastomosis provide effective treatment and reduce the risk of recurrence.
Advances in imaging techniques and surgical management have significantly improved patient outcomes. With timely diagnosis and appropriate intervention, most patients achieve successful resolution of obstruction and restoration of normal bowel function.
References
- Oren D, Atamanalp SS, Aydinli B, et al. An algorithm for the management of sigmoid colon volvulus. Am J Surg. 2007. https://pubmed.ncbi.nlm.nih.gov/17618760/
- Atamanalp SS. Sigmoid volvulus: diagnosis in 938 patients over 45.5 years. Tech Coloproctol. 2013. https://pubmed.ncbi.nlm.nih.gov/23404227/
- Lal SK, Morgenstern R, Vinjirayer EP, Matin A. Sigmoid volvulus: an update. Gastrointest Endosc Clin N Am. 2006. https://pubmed.ncbi.nlm.nih.gov/16644467/
- Perrot L, Fohlen A, Alves A, Lubrano J. Management of the colonic volvulus in 2016. J Visc Surg. 2016. https://pubmed.ncbi.nlm.nih.gov/27343625/
- Ballantyne GH. Review of sigmoid volvulus. Ann Surg. 1982. https://pubmed.ncbi.nlm.nih.gov/7055382/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge