Atrophic Glossitis: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Atrophic glossitis is a clinical condition characterized by the loss of filiform papillae, resulting in a smooth, glossy, and often erythematous tongue surface. Commonly associated with nutritional deficiencies—particularly iron, vitamin B12, and folate—it may also be linked to systemic diseases such as anemia, gastrointestinal disorders, and autoimmune conditions. Patients often present with symptoms of tongue soreness, burning sensation, and altered taste. Diagnosis is primarily clinical, supported by laboratory investigations to identify underlying etiologies. Management focuses on addressing the root cause along with symptomatic relief. This case report describes a middle-aged patient presenting with classical features of atrophic glossitis secondary to vitamin B12 deficiency, emphasizing diagnostic evaluation, therapeutic approach, and clinical outcome.
Introduction
Atrophic glossitis, also referred to as “bald tongue,” is a manifestation of underlying systemic or nutritional abnormalities. It is characterized by the atrophy of lingual papillae, giving the tongue a smooth and shiny appearance. The condition is not a disease in itself but rather a clinical sign pointing toward underlying pathology.
The most common etiological factors include deficiencies of iron, vitamin B12, and folic acid. Other causes include chronic infections, celiac disease, Sjögren’s syndrome, and adverse drug reactions. Patients may present with discomfort, burning sensation (glossodynia), or may remain asymptomatic.
Early recognition of atrophic glossitis is clinically significant, as it may be the first visible sign of systemic deficiency states. Prompt diagnosis and targeted management can lead to complete resolution and prevent long-term complications.
Case Report
Patient History
A 45-year-old female presented to the outpatient department with complaints of a persistent burning sensation of the tongue for the past 3 months. The discomfort was aggravated by spicy foods and hot beverages. She also reported fatigue, generalized weakness, and occasional dizziness.
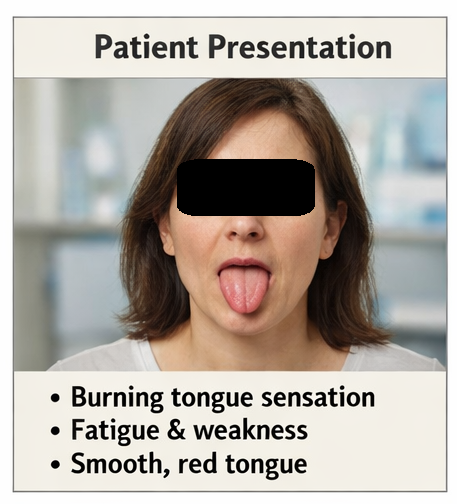
The patient noted a gradual change in the appearance of her tongue, describing it as “smooth” and “redder than usual.” There was no history of trauma, tobacco use, or alcohol consumption. Dietary history revealed a predominantly vegetarian diet with irregular intake of vitamin supplements.
There was no history of gastrointestinal disorders, chronic illnesses, or long-term medication use. Family history was non-contributory.
Clinical Examination
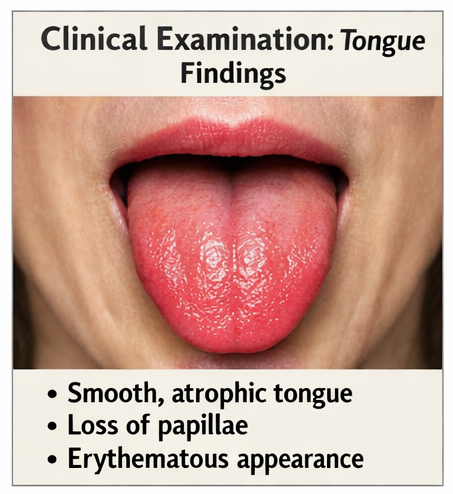
On intraoral examination, the tongue appeared:
-
Smooth and glossy with a loss of filiform papillae
-
Diffusely erythematous, particularly over the dorsal surface
-
Mild tenderness on palpation
-
No ulceration, fissures, or white plaques
The rest of the oral mucosa was normal. No angular cheilitis or mucosal lesions were observed. General physical examination revealed pallor but was otherwise unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
-
Nutritional deficiency glossitis (iron, vitamin B12, folate)
-
Geographic tongue (benign migratory glossitis)
-
Oral candidiasis (erythematous type)
-
Burning mouth syndrome
-
Lichen planus
The absence of migratory lesions, fungal plaques, or reticular patterns favored a diagnosis of atrophic glossitis.
Investigations
Laboratory Findings
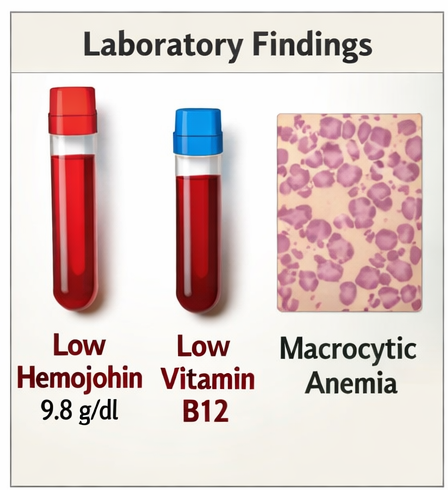
Comprehensive laboratory evaluation revealed:
-
Hemoglobin: 9.8 g/dL (low)
-
Mean corpuscular volume (MCV): Elevated
-
Serum vitamin B12: Significantly reduced
-
Serum folate: Within normal limits
-
Serum ferritin: Normal
-
Peripheral smear: Macrocytic anemia
These findings were consistent with vitamin B12 deficiency anemia.
Additional Tests
-
Thyroid function tests: Normal
-
Blood glucose levels: Normal
-
Anti-intrinsic factor antibodies: Negative
No evidence of autoimmune gastritis or endocrine abnormalities was found.
Diagnosis
Based on clinical features and laboratory findings, the diagnosis was established as:
Atrophic glossitis secondary to vitamin B12 deficiency
Management and Outcome
Initial Management
The patient was counseled regarding the underlying nutritional deficiency and its systemic implications. Dietary counseling was provided, emphasizing the inclusion of vitamin B12-rich foods and supplementation.
Pharmacological Treatment
-
Vitamin B12 supplementation:
Intramuscular cyanocobalamin injections were initiated (1000 mcg weekly for 4 weeks, followed by monthly maintenance doses). -
Oral multivitamin supplementation:
To support overall nutritional status -
Topical management:
-
Benzydamine mouthwash for symptomatic relief
-
Avoidance of irritants such as spicy foods
-

Follow-Up
At 4 weeks:
-
Reduction in burning sensation
-
Improved energy levels
-
Partial restoration of papillae
At 8 weeks:
-
Significant symptomatic relief
-
Visible improvement in tongue texture
-
Hemoglobin levels improving
At 12 weeks:
-
Near-complete resolution of glossitis
-
Normalization of vitamin B12 levels
-
No residual discomfort

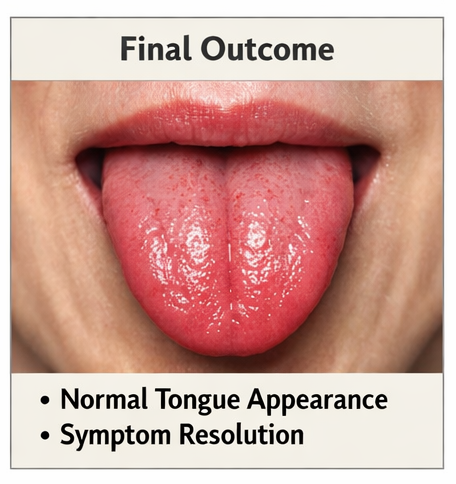
Outcome
The patient demonstrated:
-
Complete symptomatic relief
-
Restoration of normal tongue morphology
-
Improved hematological parameters
-
No recurrence at 6-month follow-up
Discussion
Atrophic glossitis is an important clinical indicator of systemic disease, particularly nutritional deficiencies. Vitamin B12 plays a crucial role in DNA synthesis and epithelial cell turnover. Deficiency leads to mucosal atrophy, particularly in rapidly dividing tissues such as the lingual epithelium.
The hallmark feature is the loss of filiform papillae, resulting in a smooth, erythematous tongue. Patients may experience burning sensation, dysgeusia, or hypersensitivity.
Etiology and Risk Factors
Common causes include:
-
Vitamin B12 deficiency
-
Iron deficiency anemia
-
Folate deficiency
-
Malabsorption syndromes
-
Chronic alcoholism
-
Medications (e.g., proton pump inhibitors, metformin)
-
Autoimmune disorders
Diagnosis
Diagnosis is based on:
-
Clinical appearance of the tongue
-
Detailed dietary and medical history
-
Laboratory investigations to identify deficiencies
Biopsy is rarely required unless malignancy or other pathology is suspected.
Management Strategies
1. Etiological Treatment
-
Correction of nutritional deficiencies
-
Management of underlying systemic conditions
2. Symptomatic Relief
-
Topical analgesics
-
Mouth rinses
-
Dietary modifications
3. Patient Education
-
Importance of balanced nutrition
-
Adherence to supplementation
-
Regular follow-up
Complications
If left untreated, atrophic glossitis may lead to:
-
Persistent discomfort
-
Difficulty in eating
-
Nutritional deterioration
-
Neurological complications (in B12 deficiency)
Prognosis
The prognosis is excellent when the underlying cause is identified and treated promptly. Most cases show complete reversal of symptoms and mucosal changes.
Conclusion
Atrophic glossitis is a clinically significant condition that often reflects underlying systemic deficiencies, particularly vitamin B12 deficiency. It presents with a characteristic smooth and erythematous tongue, often accompanied by discomfort and systemic symptoms.
Early diagnosis through clinical recognition and targeted laboratory evaluation is essential. Management focuses on correcting the underlying deficiency and providing symptomatic relief. This case underscores the importance of considering nutritional deficiencies in patients presenting with oral mucosal changes and highlights the favorable outcome with timely intervention.
References
-
Green R, Allen LH, Bjørke-Monsen AL, et al. Vitamin B12 deficiency. https://pubmed.ncbi.nlm.nih.gov/25860423/
-
Langan RC, Zawistoski KJ. Update on vitamin B12 deficiency. https://pubmed.ncbi.nlm.nih.gov/26926814/
-
Field EA, Allan RB. Review article: oral ulceration—aetiopathogenesis, clinical diagnosis and management. https://pubmed.ncbi.nlm.nih.gov/18422962/
-
Reamy BV, Derby R, Bunt CW. Common tongue conditions in primary care. https://pubmed.ncbi.nlm.nih.gov/23214284/
-
Ship JA, Chavez EM, Doerr PA, Henson BS, Sarmadi M. Reversible oral manifestations of systemic disease. https://pubmed.ncbi.nlm.nih.gov/14611518/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge