Kawasaki Disease: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Kawasaki disease is an acute, self-limited systemic vasculitis of unknown etiology that predominantly affects children under five years of age. It primarily involves medium-sized arteries, with a particular predilection for the coronary arteries, making it the leading cause of acquired heart disease in children in many parts of the world. The disease is characterized by prolonged fever, mucocutaneous inflammation, and lymphadenopathy. If left untreated, it can lead to serious cardiovascular complications, including coronary artery aneurysms. Diagnosis is mainly clinical, supported by laboratory findings and echocardiographic evaluation. Early initiation of treatment with intravenous immunoglobulin (IVIG) and aspirin significantly reduces morbidity and mortality. This case report presents a typical presentation of Kawasaki disease in a young child, highlighting clinical features, diagnostic workup, therapeutic intervention, and favorable outcome following timely management.
Introduction
Kawasaki disease is an acute febrile illness first described by Dr. Tomisaku Kawasaki in 1967. It is classified as a systemic vasculitis affecting medium-sized arteries, particularly the coronary arteries. Although the exact cause remains unknown, current evidence suggests a multifactorial etiology involving infectious triggers, genetic predisposition, and immune-mediated mechanisms.
The disease is most commonly observed in children younger than five years, with a higher incidence in males and individuals of Asian descent. Seasonal variations and clustering of cases further support a possible infectious origin.
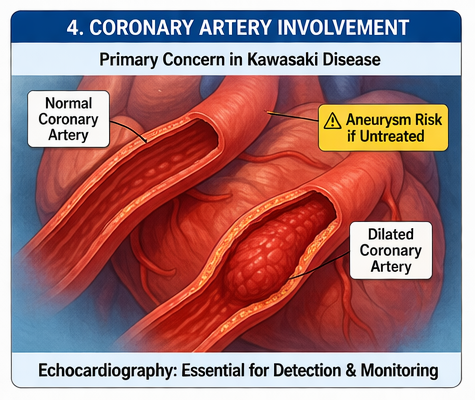
Pathophysiologically, Kawasaki disease involves widespread inflammation of blood vessels, leading to endothelial dysfunction and vascular damage. The most serious complication is coronary artery involvement, which can result in aneurysm formation, thrombosis, or myocardial ischemia.
The disease progresses through three clinical phases:
• Acute phase (1–2 weeks): Characterized by high-grade fever and inflammatory symptoms
• Subacute phase (2–4 weeks): Resolution of fever with risk of coronary artery complications
• Convalescent phase (weeks to months): Gradual normalization of clinical and laboratory parameters
Risk factors include:
• Age below 5 years
• Male gender
• Asian ethnicity
• Genetic susceptibility
• Environmental or infectious triggers
Early diagnosis is critical, as prompt treatment significantly reduces the risk of coronary artery abnormalities and improves long-term outcomes.
Case Report
Patient History
A 3-year-old male child was brought to the pediatric outpatient department with complaints of persistent high-grade fever for six days. The fever was continuous, reaching up to 39–40°C, and showed minimal response to antipyretic medications.
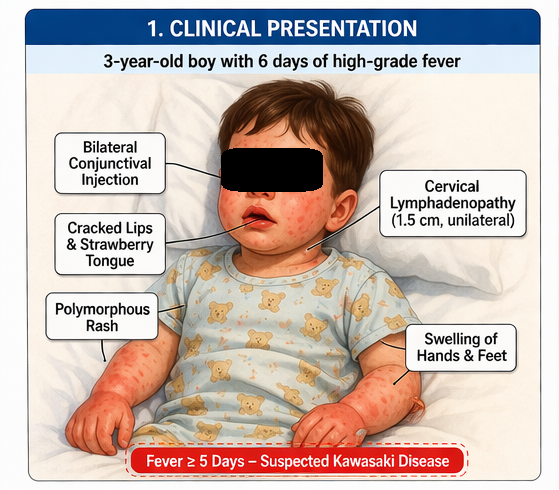
The caregiver also reported the following associated symptoms:
• Bilateral redness of eyes without discharge
• Diffuse erythematous rash over the trunk and extremities
• Swelling of hands and feet
• Cracked, dry lips and redness of oral mucosa
• Decreased appetite
• Increased irritability
There was no history of recent infection, drug exposure, or travel. Immunization history was up to date, and there was no significant past medical history.
Clinical Examination
On examination, the child appeared irritable but alert and responsive.
Vital signs were as follows:
• Temperature: 39.5°C
• Heart rate: 120 beats per minute
• Respiratory rate: 24 breaths per minute
• Blood pressure: within normal range for age
General physical examination revealed:
• Bilateral non-purulent conjunctival injection
• Dry, cracked lips and “strawberry tongue”
• Diffuse polymorphous rash over trunk
• Edema and erythema of hands and feet
• Unilateral cervical lymphadenopathy measuring approximately 1.5 cm
Systemic examination did not reveal any abnormalities in cardiovascular, respiratory, or neurological systems.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
• Viral exanthematous illness
• Scarlet fever
• Measles
• Toxic shock syndrome
• Drug hypersensitivity reaction
• Kawasaki disease
Given the persistence of fever and presence of classical mucocutaneous features, Kawasaki disease was strongly suspected.
Investigations
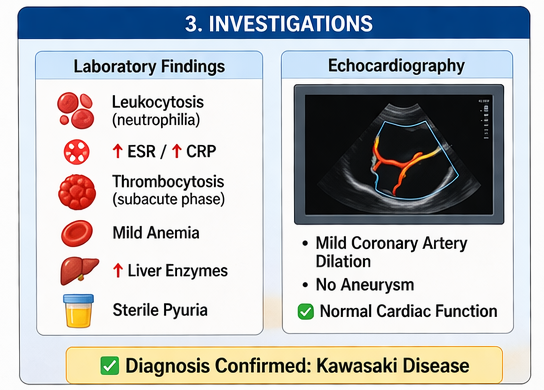
Laboratory Findings
• Complete blood count: leukocytosis with neutrophilia
• Hemoglobin: mild anemia
• Platelet count: elevated (noted during subacute phase)
• Erythrocyte sedimentation rate (ESR): elevated
• C-reactive protein (CRP): significantly elevated
• Liver function tests: mildly elevated transaminases
Urine Analysis
• Presence of sterile pyuria
Echocardiography
• Mild dilation of coronary arteries
• No evidence of aneurysm formation
• Normal cardiac function
Microbiological Tests
• Blood cultures: negative
• Viral serology: negative
These findings supported the diagnosis of Kawasaki disease while ruling out infectious causes.
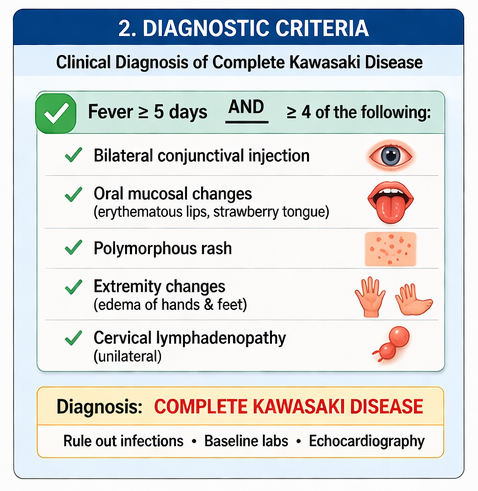
Diagnosis
Based on the presence of fever lasting more than five days along with four principal clinical features—conjunctivitis, oral mucosal changes, rash, and extremity changes—the diagnosis was confirmed as:
Complete Kawasaki Disease
Management and Outcome
Initial Management
The patient was admitted for close monitoring and initiation of treatment.
Therapeutic interventions included:
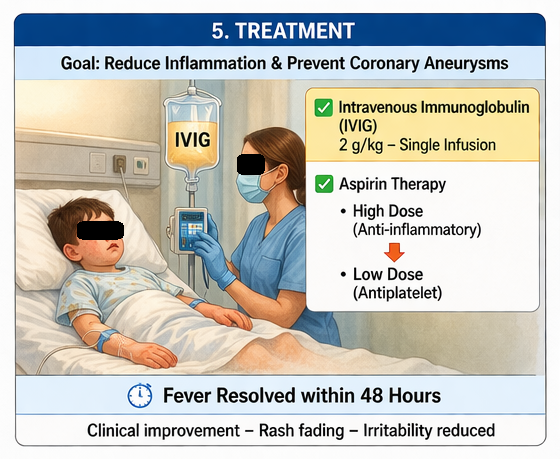
• Intravenous immunoglobulin (IVIG) at a dose of 2 g/kg administered as a single infusion
• High-dose aspirin (80–100 mg/kg/day) for anti-inflammatory effect
• Adequate hydration and supportive care
Clinical Response
The patient showed significant clinical improvement within 36–48 hours of IVIG administration:
• Fever subsided completely
• Irritability decreased
• Rash began to fade
• Oral and conjunctival changes improved
Follow-Up Management
After resolution of fever, aspirin was reduced to a low-dose regimen (3–5 mg/kg/day) for its antiplatelet effect.
Serial echocardiographic monitoring was planned to assess coronary artery status.
Outcome
At 6-week follow-up:
• The child was asymptomatic
• No coronary artery abnormalities were detected on repeat echocardiography
• Laboratory parameters normalized
• The child resumed normal daily activities
Discussion
Kawasaki disease is a significant pediatric condition due to its potential to cause long-term cardiovascular complications. Despite being self-limited, the inflammatory process can lead to serious coronary artery involvement if not treated promptly.
Diagnosis remains primarily clinical and is based on established criteria, including prolonged fever and characteristic mucocutaneous findings. However, incomplete or atypical presentations may pose diagnostic challenges, particularly in infants.
Laboratory findings typically reflect systemic inflammation and include elevated ESR, CRP, leukocytosis, and thrombocytosis. Sterile pyuria and mild liver enzyme elevation are also common.
Echocardiography plays a crucial role in both diagnosis and follow-up by identifying coronary artery abnormalities such as dilation or aneurysms. It is recommended at diagnosis and repeated during follow-up to monitor progression.
The cornerstone of treatment is early administration of IVIG, ideally within the first 10 days of illness. IVIG has been shown to significantly reduce the risk of coronary artery aneurysm formation. Aspirin is used initially for its anti-inflammatory properties and later for its antiplatelet effects.
In cases resistant to initial IVIG therapy, additional treatments such as corticosteroids or biologic agents (e.g., infliximab) may be considered.
Prognosis is generally excellent when treated early. However, patients with coronary artery involvement require long-term follow-up due to the risk of complications such as thrombosis or myocardial ischemia.
Conclusion
Kawasaki disease is an important cause of pediatric vasculitis with the potential for serious cardiovascular complications if not recognized and treated promptly. It typically presents with prolonged fever and characteristic mucocutaneous features, requiring a high index of clinical suspicion for early diagnosis.
Timely administration of intravenous immunoglobulin and aspirin significantly reduces the risk of coronary artery involvement and improves overall outcomes. Echocardiographic monitoring is essential for detecting cardiac complications and guiding long-term management.
This case highlights the importance of early recognition and intervention, demonstrating that prompt and appropriate treatment can lead to complete recovery without long-term sequelae. Continued awareness among clinicians is crucial to ensure optimal patient outcomes and prevent potentially life-threatening complications.
References
-
McCrindle BW, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease. https://pubmed.ncbi.nlm.nih.gov/28356445/
-
Newburger JW, et al. Kawasaki Disease. https://pubmed.ncbi.nlm.nih.gov/28538148/
-
Rowley AH. Kawasaki disease: novel insights into etiology and genetic susceptibility. https://pubmed.ncbi.nlm.nih.gov/28798006/
-
Sundel RP. Kawasaki disease: epidemiology and pathogenesis. https://pubmed.ncbi.nlm.nih.gov/23445772/
-
Eleftheriou D, et al. Management of Kawasaki disease. https://pubmed.ncbi.nlm.nih.gov/26655288/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge