Median Canaliform Nail Dystrophy (Heller): Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Median canaliform nail dystrophy (MCND), also known as Heller’s dystrophy, is a rare, benign nail disorder characterized by a central longitudinal groove with lateral ridging resembling a “fir-tree” pattern. The condition most commonly affects the thumbnails and is often associated with repetitive trauma to the nail matrix, although idiopathic cases are also reported. Patients are usually asymptomatic, and the condition is primarily a cosmetic concern. Diagnosis is clinical, supported by characteristic nail morphology, and rarely requires histopathological confirmation. Management focuses on eliminating causative factors, behavioral modification, and topical therapies. This case report describes a middle-aged patient presenting with classical features of MCND, highlighting diagnostic considerations, treatment approach, and clinical outcome.
Introduction
Median canaliform nail dystrophy is an uncommon nail plate disorder first described by Heller. It is characterized by a longitudinal midline split or canal in the nail plate, accompanied by transverse ridges that extend laterally, giving a distinctive fir-tree appearance. The condition most frequently involves the thumbnails but may occasionally affect other fingernails.
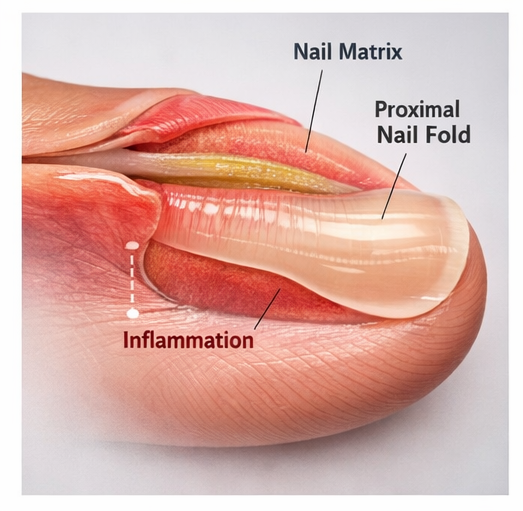
The exact pathogenesis remains unclear; however, repeated microtrauma to the nail matrix—often due to habitual picking or manipulation—is considered a primary contributing factor. Other associations include the use of systemic retinoids and underlying psychological stress.
Although MCND is a benign condition, it can cause significant cosmetic concern and anxiety for patients. Differentiating it from other nail dystrophies such as onychotillomania, nail psoriasis, or lichen planus is essential for appropriate management. Early recognition and intervention can prevent progression and improve outcomes.
Case Report
Patient History
A 32-year-old female presented to the dermatology outpatient department with concerns regarding an abnormal appearance of her thumbnails for the past 8 months.

She reported the gradual development of a central groove on both thumbnails, which progressively deepened over time.

There was no associated pain, discharge, or nail discoloration. The patient denied any history of trauma but admitted to frequent subconscious picking and rubbing of the proximal nail fold during periods of stress.
There was no history of systemic illness, dermatological conditions, or use of systemic medications such as retinoids. Family history was non-contributory.
Clinical Examination
On examination, both thumbnails showed:
- A central longitudinal groove extending from the proximal nail fold to the distal edge
- Multiple transverse ridges radiating laterally, forming a fir-tree pattern
- Intact nail folds without inflammation
- No signs of onycholysis, subungual hyperkeratosis, or pigmentation
Other fingernails and toenails were normal. There were no cutaneous lesions suggestive of psoriasis or lichen planus.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
- Onychotillomania
- Nail psoriasis
- Lichen planus of the nail
- Trachyonychia
- Habit-tic deformity
The absence of inflammation, scaling, and systemic involvement, along with the characteristic pattern, favored a diagnosis of MCND.
Investigations
Laboratory Findings
Routine laboratory investigations were within normal limits:
- Complete blood count: Normal
- Thyroid function tests: Normal
- Blood glucose levels: Normal
No systemic abnormalities were identified.
Dermoscopic Examination
Dermoscopy of the nail plate revealed:
- Central canal-like depression
- Symmetrical transverse ridging
- Absence of vascular abnormalities
These findings supported the clinical diagnosis.
Histopathological Examination
Histopathological evaluation was not performed, as the diagnosis was established clinically and invasiveness was unnecessary.
Diagnosis
Based on clinical and dermoscopic findings, the diagnosis was established as:
Median Canaliform Nail Dystrophy (Heller)
Management and Outcome
Initial Management
The patient was counseled regarding the benign nature of the condition and its association with repetitive trauma.
Behavioral modification strategies were emphasized:
- Avoidance of nail picking and manipulation
- Stress management techniques
- Use of protective barriers (e.g., gloves if needed)

Pharmacological Treatment
Topical therapy was initiated with a focus on reducing inflammation at the nail matrix and promoting normalization of nail growth:
- Topical tacrolimus 0.1% ointment was applied to the proximal nail fold once daily, targeting subclinical inflammation and aiding in restoration of matrix function. The patient was advised to apply a thin layer with gentle massage to enhance absorption and avoid occlusion unless specifically recommended.
- Emollients were prescribed to maintain adequate nail and periungual hydration, improve nail plate flexibility, and reduce brittleness, thereby minimizing further mechanical damage.
- In addition, the patient was counseled on the regular use of barrier repair creams to strengthen the periungual skin and reduce susceptibility to repetitive microtrauma.
- The importance of treatment adherence was emphasized, as topical therapies in nail disorders require prolonged and consistent application to achieve visible improvement due to the slow rate of nail growth.
Follow-Up
At 6 weeks:
- Reduction in progression of nail dystrophy
- Improved patient compliance with behavioral changes
At 3 months:
- Partial improvement in nail appearance
- Reduced depth of the central groove
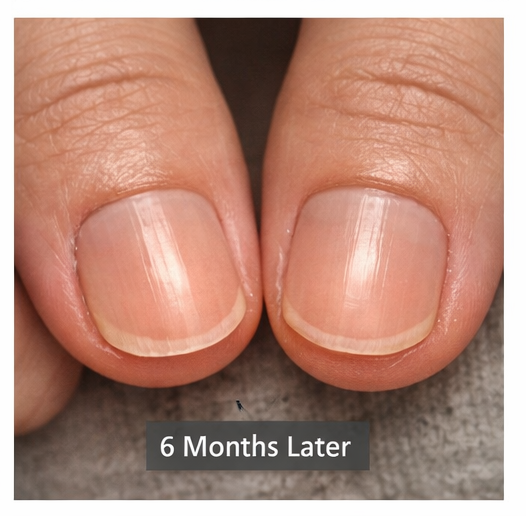
At 6 months:
- Significant cosmetic improvement
- No new nail involvement
Outcome
The patient demonstrated:
- Stabilization of nail changes
- Gradual improvement in nail morphology
- No recurrence with continued behavioral adherence
Discussion
Median canaliform nail dystrophy is a rare but distinctive nail disorder with a characteristic clinical appearance. The pathogenesis is believed to involve temporary disruption of nail matrix keratinization, often triggered by repetitive trauma or habitual behaviors.
Patients are typically asymptomatic, and diagnosis is primarily clinical. Dermoscopy can aid in distinguishing MCND from other nail pathologies by highlighting the symmetrical canal and ridging pattern.
Risk Factors
Key contributing factors include:
- Repetitive trauma to the nail matrix
- Habitual nail picking (onychotillomania)
- Psychological stress
- Use of systemic retinoids
Diagnosis
Diagnosis is based on:
- Characteristic clinical morphology
- History of repetitive trauma or behavioral habits
Histopathology is rarely required but may show matrix disruption.
Management Strategies
Behavioral Modification
- Cornerstone of treatment
- Includes habit reversal techniques
Topical Therapy
- Tacrolimus or corticosteroids may help reduce inflammation and matrix damage
Other Therapies
- Intralesional steroids (rarely used)
- Avoidance of triggering medications
Complications
- Persistent cosmetic deformity
- Psychological distress
No malignant transformation is associated with this condition.
Prognosis
The prognosis is generally favorable with appropriate behavioral modification and treatment. However, recurrence may occur if triggering habits persist.
Conclusion
Median canaliform nail dystrophy is a benign nail condition characterized by a distinctive central canal and lateral ridging, most commonly affecting the thumbnails. It is often associated with repetitive trauma to the nail matrix, particularly due to habitual behaviors.
Diagnosis is primarily clinical, and management focuses on behavioral modification and topical therapy. Early recognition and patient counseling are crucial to prevent progression and improve cosmetic outcomes. This case highlights the importance of identifying subtle behavioral triggers in nail disorders to ensure effective management and favorable prognosis.
References
- Haneke E. Nail disorders: diagnosis and management. https://pubmed.ncbi.nlm.nih.gov/20159316/
- Piraccini BM, Alessandrini A. Onychotillomania and nail dystrophies. https://pubmed.ncbi.nlm.nih.gov/25828710/
- Tosti A, Piraccini BM, Iorizzo M. Dermoscopy of nail disorders. https://pubmed.ncbi.nlm.nih.gov/19076872/
- Richert B, Andre J. Nail disorders in dermatology. https://pubmed.ncbi.nlm.nih.gov/21146736/
- de Berker D. Nail anatomy and physiology. https://pubmed.ncbi.nlm.nih.gov/17999803/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge