Hairy Mole (Congenital Melanocytic Nevus): Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Congenital melanocytic nevus (CMN), commonly referred to as a hairy mole, is a benign pigmented lesion present at birth or shortly thereafter, resulting from proliferation of melanocytes. These lesions vary in size and may be associated with hypertrichosis, surface irregularity, and progressive changes over time. While most CMNs remain benign, larger lesions carry a potential risk of malignant transformation and psychosocial impact. Diagnosis is primarily clinical, supported by dermoscopic evaluation. Management ranges from observation to surgical excision depending on risk profile and patient preference. This case report describes a young adult with a congenital hairy mole, highlighting clinical presentation, diagnostic approach, management, and favorable outcome following surgical intervention.
Introduction
Congenital melanocytic nevus is a developmental anomaly arising due to aberrant proliferation of melanocytes during embryogenesis. These lesions are typically present at birth or become evident within the first few months of life. CMNs are classified based on projected adult size into small, medium, and large (giant) nevi, with increasing size correlating with higher risk of complications.
Clinically, CMNs present as well-demarcated pigmented patches or plaques that may vary in color from light brown to dark black. Many lesions exhibit hypertrichosis, giving rise to the term “hairy mole.” Over time, they may undergo changes such as thickening, nodularity, or darkening, which require careful evaluation.
Although the majority of CMNs are benign, concerns include malignant transformation into melanoma, particularly in large lesions, as well as cosmetic and psychological implications. Early diagnosis, risk stratification, and appropriate follow-up are essential components of management.
Case Report
Patient History
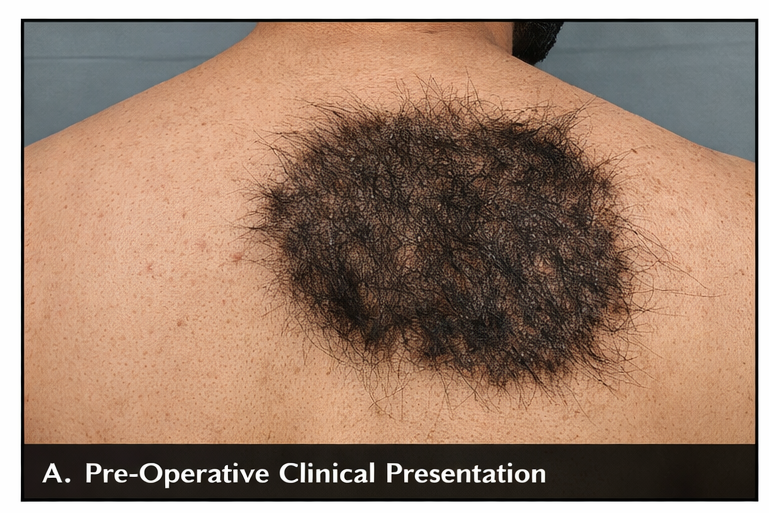
A 24-year-old male presented to the dermatology outpatient department with a pigmented lesion over the left shoulder present since birth. The patient reported gradual increase in size proportional to body growth.
He expressed cosmetic concerns and occasional mild itching but denied pain, bleeding, ulceration, or rapid changes in the lesion. There was no history of trauma or similar lesions elsewhere on the body.
The patient had no significant past medical history and was not on any long-term medications. Family history was negative for melanoma or other skin malignancies.
Clinical Examination
On examination, the patient was afebrile and hemodynamically stable.
Local examination revealed:
• A well-defined hyperpigmented plaque measuring approximately 10 × 7 cm
• Irregular but clearly demarcated borders
• Surface showing mild thickening and uneven texture
• Dense, coarse terminal hair over the lesion
• No ulceration, bleeding, or signs of secondary infection
There was no regional lymphadenopathy. Systemic examination was unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on clinical findings, the following conditions were considered:
• Congenital melanocytic nevus
• Becker’s nevus
• Pigmented epidermal nevus
• Nevus spilus
• Melanoma (to be ruled out)
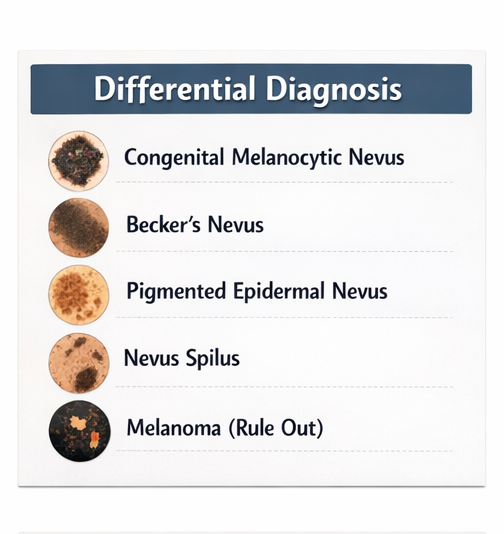
The congenital onset, pigmentation pattern, and presence of hypertrichosis strongly supported the diagnosis of CMN.
Investigations
Dermoscopy
Dermoscopy revealed:
• Homogeneous pigmentation with globular and reticular patterns
• Uniform distribution without atypical structures
• Absence of irregular vascular patterns

Laboratory Findings
Routine investigations were within normal limits.
No imaging studies were required. Skin biopsy was not performed due to the absence of suspicious features.
Diagnosis
Based on clinical and dermoscopic evaluation, the diagnosis was established as:
Congenital Melanocytic Nevus (Hairy Mole)
Management and Outcome
Initial Management
The patient was counseled regarding the benign nature of the lesion, potential risks, and available treatment options.
Management plan included:
• Regular clinical monitoring
• Sun protection measures
• Elective surgical excision for cosmetic improvement
Surgical Management
The patient opted for surgical excision. The lesion was excised under appropriate surgical conditions with adequate margins, followed by primary closure.

Follow-Up
At one-week follow-up:
• Wound healing was satisfactory
• No infection or complications
At one-month follow-up:
• Complete healing observed
• Acceptable cosmetic outcome
At three-month follow-up:
• No recurrence
• Patient reported high satisfaction

Outcome
The patient demonstrated:
• Successful removal of the lesion
• Improved cosmetic appearance
• No evidence of malignancy or recurrence
Discussion
Congenital melanocytic nevi are benign proliferations of melanocytes that arise during fetal development. The lesions result from abnormal migration and growth of melanocyte precursors derived from the neural crest.
The clinical presentation depends on the size and location of the nevus. Small and medium CMNs are more common and generally carry a low risk of malignant transformation, whereas large or giant nevi are associated with higher risk. The presence of hair, irregular surface, and pigmentation are characteristic features.
Diagnosis is primarily clinical, with dermoscopy serving as a valuable adjunct tool to assess pigment patterns and identify atypical features. Biopsy is reserved for lesions showing suspicious changes such as rapid growth, ulceration, or color variation.
Management is individualized and depends on several factors including size, location, cosmetic concerns, and risk of malignancy. Options include:
• Observation with regular follow-up
• Surgical excision for cosmetic or preventive purposes
Surgical removal offers definitive treatment but may be associated with scarring. In selected cases, staged excision or reconstructive procedures may be required.
Complications associated with CMN include:
• Malignant transformation into melanoma (rare in small lesions)
• Psychological distress due to cosmetic appearance
• Local irritation or itching
Preventive strategies include:
• Regular dermatological evaluation
• Sun protection
• Early reporting of changes such as bleeding, ulceration, or rapid growth
The prognosis for small and medium CMNs is excellent, particularly with regular monitoring and timely intervention when required.
Conclusion
Congenital melanocytic nevus (hairy mole) is a benign pigmented lesion present since birth, often associated with hypertrichosis and gradual growth. Diagnosis is primarily clinical, supported by dermoscopy. While most lesions remain benign, monitoring is essential to detect any suspicious changes. Management should be individualized, with surgical excision offering good cosmetic and clinical outcomes in selected cases. This case underscores the importance of early evaluation, patient counseling, and appropriate management in achieving favorable results.
References
- Krengel S, Scope A, Dusza SW, et al. New recommendations for the categorization of cutaneous melanocytic nevi. https://pubmed.ncbi.nlm.nih.gov/20159388/
- Bett BJ. Large or multiple congenital melanocytic nevi: occurrence of cutaneous melanoma. https://pubmed.ncbi.nlm.nih.gov/16713459/
- Marghoob AA, Borrego JP, Halpern AC. Congenital melanocytic nevi: treatment modalities and management options. https://pubmed.ncbi.nlm.nih.gov/15113215/
- Kinsler VA, O’Hare P, Bulstrode N. Melanoma in congenital melanocytic naevi. https://pubmed.ncbi.nlm.nih.gov/22296263/
- Price HN, Schaffer JV. Congenital melanocytic nevi—when to worry and how to treat. https://pubmed.ncbi.nlm.nih.gov/23047185/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge