Wernicke Encephalopathy: Clinical Presentation, Diagnostic Challenges, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
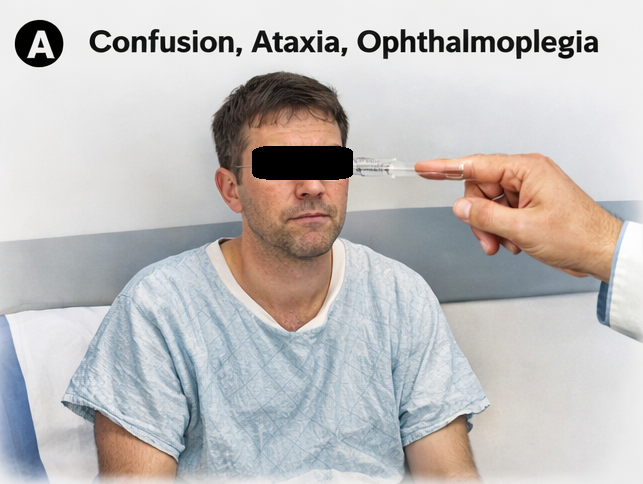
Wernicke encephalopathy is an acute, life-threatening neurological disorder caused by thiamine (vitamin B1) deficiency. It is classically characterized by the triad of confusion, ophthalmoplegia, and ataxia; however, this triad is present in only a minority of cases, often leading to underdiagnosis. The condition is most commonly associated with chronic alcohol use but may also occur in malnutrition, prolonged vomiting, and systemic illnesses.
We report a case of a 42-year-old male presenting with altered mental status, gait instability, and visual disturbances. Magnetic resonance imaging (MRI) findings, along with clinical suspicion, confirmed the diagnosis of Wernicke encephalopathy. Prompt treatment with intravenous thiamine resulted in significant neurological improvement. This case underscores the importance of early recognition and timely intervention to prevent irreversible complications such as Korsakoff syndrome.
Introduction
Wernicke encephalopathy (WE) is a neurological emergency resulting from thiamine deficiency, which impairs cerebral energy metabolism. It is most frequently associated with chronic alcoholism but can also occur in conditions such as malnutrition, hyperemesis gravidarum, malignancy, and post-bariatric surgery states.
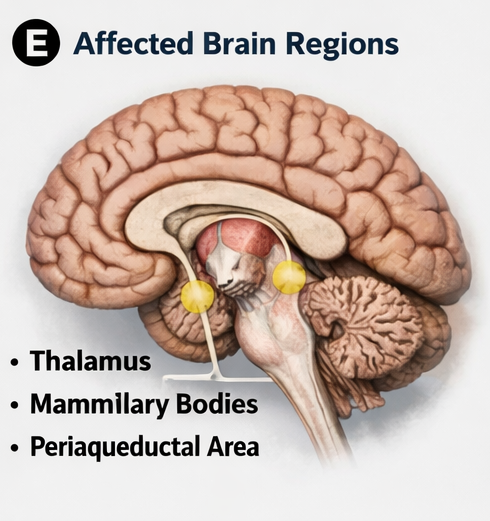
Thiamine plays a critical role as a cofactor in carbohydrate metabolism, particularly in pathways such as the Krebs cycle and pentose phosphate pathway. Deficiency leads to neuronal injury, particularly in regions with high metabolic demand such as the mammillary bodies, thalamus, and brainstem.
The classical triad of WE includes:
- Encephalopathy (confusion)
- Oculomotor dysfunction
- Gait ataxia
However, fewer than one-third of patients present with all three features, making clinical diagnosis challenging. Delayed treatment may result in irreversible neurological damage or progression to Korsakoff syndrome, characterized by chronic memory impairment.
This case report highlights the clinical presentation, diagnostic approach, and management of Wernicke encephalopathy with favorable outcomes following early intervention.
Case Report
Patient History
A 42-year-old male presented to the emergency department with progressive confusion, difficulty walking, and blurred vision for 5 days. The patient had a history of chronic alcohol use for over 15 years, with poor nutritional intake.
There was no history of trauma, seizures, or prior neurological illness. The patient’s family reported recent behavioral changes, including disorientation and memory lapses.
Clinical Examination
On examination, the patient was disoriented to time and place.
Key findings included:
- Altered mental status with confusion
- Horizontal nystagmus and bilateral lateral rectus weakness
- Broad-based, unsteady gait (ataxia)
- Mild hypotension and signs of malnutrition
Neurological examination showed no focal motor deficits. Reflexes were preserved, and there were no signs of meningeal irritation.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
- Wernicke encephalopathy
- Alcohol withdrawal delirium
- Hepatic encephalopathy
- Intracranial pathology (e.g., stroke, tumor)
- Nutritional deficiency-related neuropathy
The combination of chronic alcoholism, confusion, and ocular signs strongly suggested WE.
Investigations
Laboratory Findings
- Mild anemia
- Electrolyte imbalance (hypomagnesemia)
- Elevated liver enzymes
- Low serum thiamine levels
Radiological Evaluation
MRI of the brain revealed:
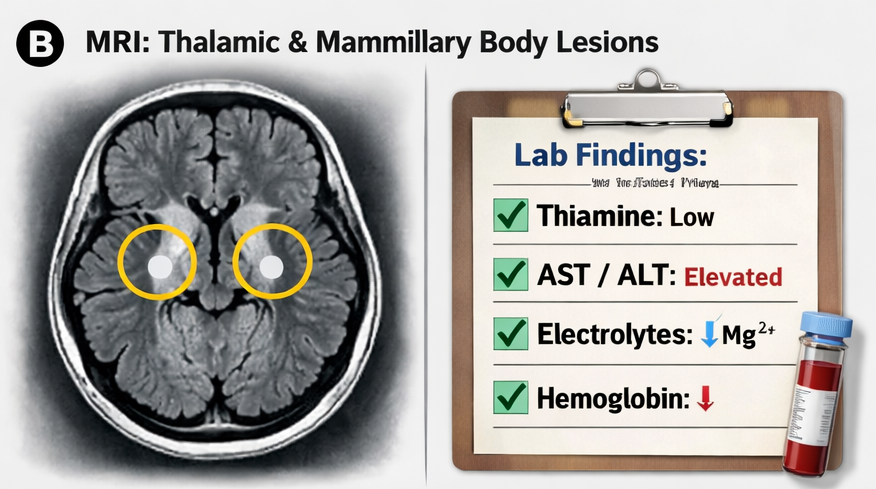
- Symmetrical hyperintensities in the medial thalami
- Involvement of mammillary bodies
- Periaqueductal gray matter changes
These findings were consistent with Wernicke encephalopathy.
Computed tomography (CT) was unremarkable and less sensitive for early detection.
Diagnosis
Based on the patient’s clinical presentation—characterized by confusion, gait ataxia, and ophthalmoplegia—along with supportive MRI findings showing symmetrical signal alterations in the mammillary bodies, medial thalami, and periaqueductal region, a diagnosis of Wernicke encephalopathy was established.
The underlying etiology was chronic alcohol use leading to severe thiamine (vitamin B1) deficiency, resulting in impaired cerebral energy metabolism and neuronal injury. These neuroimaging findings, in conjunction with the clinical triad, are highly suggestive of this acute neuropsychiatric syndrome.
Early recognition is critical, as delayed treatment can result in progression to Korsakoff syndrome, characterized by irreversible memory impairment and confabulation. Prompt initiation of high-dose parenteral thiamine is essential and can lead to significant clinical improvement, particularly in ocular and gait abnormalities, while cognitive recovery may be variable.
Management and Outcome
Management Strategy
Medical Treatment
Immediate treatment was initiated without waiting for laboratory confirmation:
- High-dose intravenous thiamine (500 mg TID for 3 days)
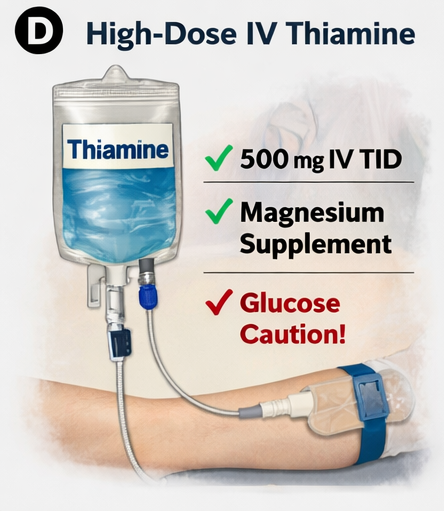
- Followed by 250 mg IV daily for 5 days
- Transition to oral thiamine supplementation
- Magnesium supplementation (to facilitate thiamine utilization)
- Supportive care and hydration
Importantly, thiamine was administered before glucose infusion to prevent exacerbation of symptoms.
Rehabilitation
- Nutritional rehabilitation with a balanced diet
- Alcohol cessation counseling
- Physiotherapy for gait improvement
- Cognitive support and monitoring
Follow-Up and Outcome
At 1 week:
- Improvement in confusion
- Reduction in nystagmus
At 4 weeks:
- Significant recovery in gait
- Improved coordination
At 8 weeks:
- Near-complete neurological recovery
- Mild residual memory deficits
At 12 weeks:
- Independent ambulation
- No progression to Korsakoff syndrome

Discussion
Pathophysiology
Thiamine deficiency disrupts cerebral glucose metabolism, leading to:
- Reduced ATP production
- Neuronal damage
- Cytotoxic and vasogenic edema
Brain regions with high metabolic demand are particularly vulnerable.
Diagnostic Challenges
WE is frequently underdiagnosed due to:
- Incomplete clinical triad
- Overlap with alcohol-related disorders
- Non-specific early symptoms
MRI is the most sensitive imaging modality but should not delay treatment.
Treatment Considerations
Early treatment is critical and should be initiated based on clinical suspicion.
Key principles include:
- Immediate high-dose parenteral thiamine
- Correction of electrolyte imbalances
- Avoidance of glucose before thiamine
Delayed treatment increases risk of:
- Korsakoff syndrome
- Permanent cognitive impairment
Complications
Potential complications include:
- Korsakoff syndrome
- Persistent memory deficits
- Gait abnormalities
- Coma (in severe cases)
Prognosis
Prognosis depends on:
- Timing of treatment
- Severity of deficiency
Early-treated patients often show significant recovery, while delayed cases may develop irreversible damage.
Conclusion
Wernicke encephalopathy is a medical emergency that requires a high index of clinical suspicion, particularly in patients with risk factors such as chronic alcohol use and malnutrition. This case demonstrates that prompt administration of intravenous thiamine can lead to rapid and substantial neurological recovery.
Early diagnosis, appropriate imaging, and timely treatment are essential in preventing irreversible complications such as Korsakoff syndrome. Clinician awareness and proactive management remain critical to improving patient outcomes in this potentially reversible condition.
References
- Sechi, G., & Serra, A. (2007). Wernicke's encephalopathy: New clinical settings and recent advances in diagnosis and management. The Lancet Neurology, 6(5), 442–455. https://doi.org/10.1016/S1474-4422(07)70104-7
- National Center for Biotechnology Information. (2023). Wernicke encephalopathy. StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK470344/
- Harper, C. (2009). The neuropathology of alcohol-related brain damage. Alcohol and Alcoholism, 44(2), 136–140. https://academic.oup.com/alcalc/article/44/2/136/134180
- Oudman, E., et al. (2019). Wernicke’s encephalopathy in non-alcoholic patients: A systematic review. Journal of Neurology, Neurosurgery & Psychiatry, 90(5), 561–567. https://jnnp.bmj.com/content/90/5/561
- Latt, N., & Dore, G. (2014). Thiamine in the treatment of Wernicke encephalopathy in patients with alcohol use disorders. Internal Medicine Journal, 44(9), 911–915. https://onlinelibrary.wiley.com/doi/full/10.1111/imj.12522
- Radiopaedia. (n.d.). Wernicke encephalopathy. https://radiopaedia.org/articles/wernicke-encephalopathy
- Medscape. (n.d.). Wernicke encephalopathy clinical presentation. https://emedicine.medscape.com/article/794583-overview
- Victor, M., Adams, R. D., & Collins, G. H. (1989). The Wernicke-Korsakoff Syndrome. F.A. Davis Company.
- Cook, C. C., et al. (1998). Wernicke’s encephalopathy in the UK: Under-recognition and under-treatment. Alcohol and Alcoholism, 33(5), 542–545.
- Elsevier. (n.d.). Wernicke encephalopathy overview. https://www.sciencedirect.com/topics/medicine-and-dentistry/wernicke-encephalopathy
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge