Barrett’s Esophagus: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Barrett’s esophagus is a premalignant condition characterized by the replacement of normal stratified squamous epithelium of the distal esophagus with specialized intestinal metaplasia. It is strongly associated with chronic gastroesophageal reflux disease (GERD) and represents a significant risk factor for esophageal adenocarcinoma. The clinical presentation may range from typical reflux symptoms to asymptomatic disease detected incidentally during endoscopy. Diagnosis is established through endoscopic visualization and histopathological confirmation. Management includes acid suppression therapy, endoscopic surveillance, and in selected cases, endoscopic eradication therapies. This case report describes a middle-aged patient with chronic reflux symptoms who was diagnosed with Barrett’s esophagus, highlighting clinical features, diagnostic approach, treatment, and outcome.
Introduction
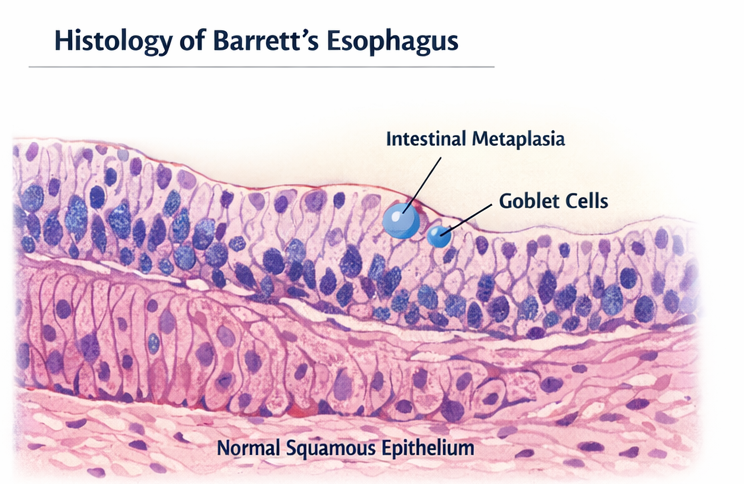
Barrett’s esophagus is a condition in which the normal squamous lining of the distal esophagus is replaced by columnar epithelium containing goblet cells, a process known as intestinal metaplasia. This transformation occurs as an adaptive response to chronic acid exposure from gastroesophageal reflux.
The condition is clinically significant due to its association with an increased risk of progression to esophageal adenocarcinoma. The annual risk of progression is relatively low but warrants surveillance due to the poor prognosis associated with advanced esophageal cancer.
Barrett’s esophagus is more commonly seen in middle-aged and older adults, particularly males, and is associated with risk factors such as chronic GERD, obesity, smoking, and hiatal hernia. Early detection and appropriate management are essential to prevent dysplastic progression and malignancy.
Case Report
Patient History
A 45-year-old male presented to the outpatient department with complaints of persistent heartburn and regurgitation for the past 5 years. The symptoms were more pronounced after meals and while lying down. He also reported occasional dysphagia to solid foods over the past 3 months.
The patient had been self-medicating with over-the-counter antacids with partial relief. There was no history of hematemesis, melena, or significant weight loss.
He had a history of obesity (BMI: 30 kg/m²) and was a chronic smoker (10 pack-years). There was no known history of gastrointestinal malignancy in the family.
Clinical Examination
On examination, the patient was hemodynamically stable. General physical examination was unremarkable.
Systemic examination revealed:
- Mild epigastric tenderness
- No organomegaly
- No lymphadenopathy
The rest of the examination was within normal limits.
Clinical Evaluation
Differential Diagnosis
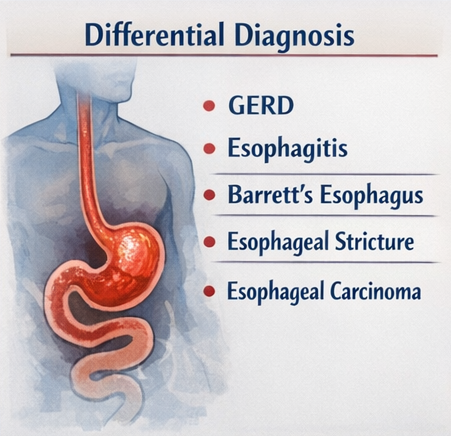
Based on the presenting symptoms, the following differential diagnoses were considered:
- Chronic gastroesophageal reflux disease (GERD)
- Esophagitis (erosive or non-erosive)
- Barrett’s esophagus
- Esophageal stricture
- Esophageal carcinoma
Chronicity of symptoms and new-onset dysphagia raised concern for complications of GERD, including Barrett’s esophagus.
Investigations
Laboratory Findings
Routine laboratory investigations were within normal limits:
- Hemoglobin: Normal
- Liver and renal function tests: Normal
- No evidence of anemia or systemic inflammation
Upper Gastrointestinal Endoscopy
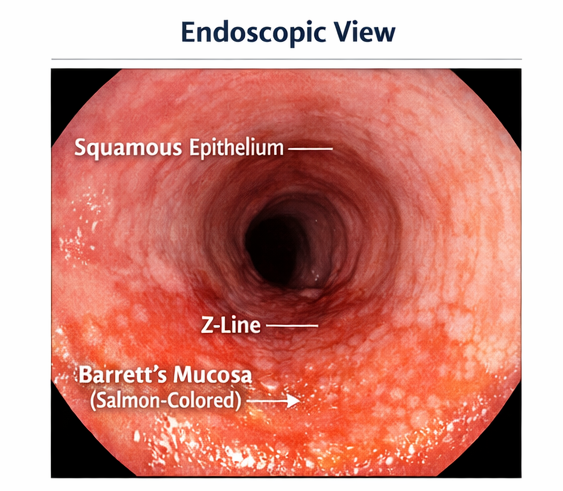
Upper GI endoscopy revealed:
- Salmon-colored mucosa extending approximately 3 cm above the gastroesophageal junction
- Irregular Z-line
- No visible ulceration or mass lesion
These findings were suggestive of Barrett’s esophagus.
Histopathological Examination
Multiple biopsies were taken from the suspected area.
Histopathology showed:
- Columnar epithelium with goblet cells
- Features consistent with specialized intestinal metaplasia
- No evidence of dysplasia
Additional Evaluation
- 24-hour pH monitoring (optional) showed increased acid exposure
- Esophageal manometry was within normal limits
Diagnosis
Based on endoscopic and histopathological findings, the diagnosis was established as:
Non-dysplastic Barrett’s Esophagus
Management and Outcome
Initial Management
The patient was counseled regarding the condition, its premalignant potential, and the importance of long-term follow-up.
Lifestyle modifications were advised:
- Weight reduction
- Smoking cessation
- Avoidance of trigger foods (spicy, fatty foods, caffeine)
- Elevation of the head end of the bed
Pharmacological Treatment
- Proton pump inhibitor (PPI): Omeprazole 40 mg once daily
- Antacids as needed for symptomatic relief
Follow-Up
At 4 weeks:
- Significant reduction in heartburn and regurgitation
- Improvement in quality of life
At 3 months:
- Complete resolution of dysphagia
- Good compliance with lifestyle modifications
At 1 year (Surveillance Endoscopy):
- No progression of Barrett’s segment
- No evidence of dysplasia
Outcome
The patient demonstrated:
- Symptomatic improvement
- Stable Barrett’s segment
- No progression to dysplasia or malignancy
Regular surveillance was planned every 3–5 years as per guidelines.
Discussion
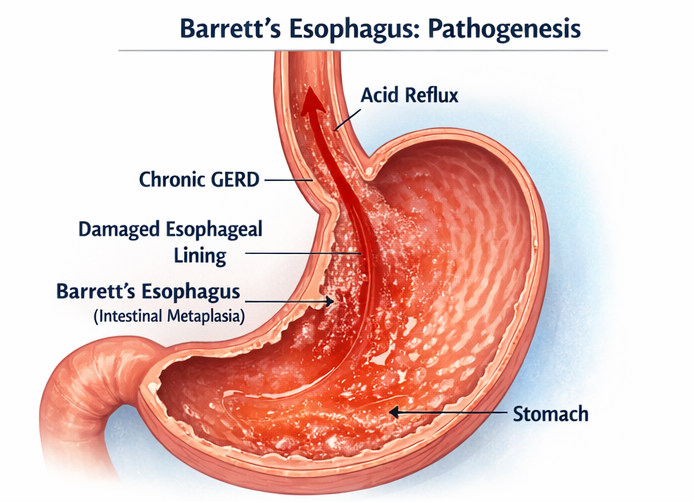
Barrett’s esophagus is a well-recognized complication of chronic GERD and represents a key risk factor for esophageal adenocarcinoma. The pathogenesis involves chronic exposure of esophageal mucosa to gastric acid and bile, leading to metaplastic transformation.
Patients may present with classic reflux symptoms such as heartburn and regurgitation, although some individuals remain asymptomatic. Alarm symptoms such as dysphagia, weight loss, or bleeding warrant prompt evaluation.
Risk Factors
Major risk factors include:
- Chronic GERD
- Male gender
- Obesity (especially central obesity)
- Smoking
- Age >50 years
- Hiatal hernia
Diagnosis
Diagnosis requires both:
- Endoscopic findings (salmon-colored mucosa)
- Histological confirmation (intestinal metaplasia with goblet cells)
The Prague classification is often used to describe the extent of Barrett’s esophagus.
Surveillance and Progression
Barrett’s esophagus progresses through a sequence:
- Non-dysplastic Barrett’s
- Low-grade dysplasia
- High-grade dysplasia
- Esophageal adenocarcinoma
Surveillance intervals depend on the presence and grade of dysplasia.
Management Strategies
Medical Management
- Proton pump inhibitors (PPIs) are the cornerstone
- They reduce acid exposure and may decrease progression risk
Endoscopic Therapy
Indicated in dysplastic Barrett’s:
- Radiofrequency ablation (RFA)
- Endoscopic mucosal resection (EMR)
Surgical Management
- Fundoplication may be considered in selected GERD patients
Complications
Potential complications include:
- Esophageal adenocarcinoma
- Esophageal strictures
- Ulceration
Prevention
Preventive strategies include:
- Early treatment of GERD
- Lifestyle modification
- Regular surveillance in high-risk patients
Prognosis
The prognosis is generally favorable in patients with non-dysplastic Barrett’s esophagus when appropriately managed and monitored. Early detection significantly reduces the risk of malignant transformation.
Conclusion
Barrett’s esophagus is an important premalignant condition arising from chronic gastroesophageal reflux. It often presents with long-standing reflux symptoms and may be complicated by dysphagia or other alarm features. Diagnosis relies on endoscopic visualization and histopathological confirmation of intestinal metaplasia.
Management focuses on acid suppression, lifestyle modification, and regular surveillance to detect early dysplastic changes. Most patients with non-dysplastic Barrett’s esophagus have a favorable outcome with appropriate treatment and follow-up. This case underscores the importance of early evaluation in patients with chronic GERD symptoms to prevent progression to esophageal adenocarcinoma.
References
- Spechler SJ, Souza RF. Barrett’s esophagus. https://pubmed.ncbi.nlm.nih.gov/24290466/
- Shaheen NJ, Falk GW, Iyer PG, et al. ACG Clinical Guideline: Diagnosis and Management of Barrett’s Esophagus. https://pubmed.ncbi.nlm.nih.gov/26526079/
- Fitzgerald RC, di Pietro M, Ragunath K, et al. British Society of Gastroenterology guidelines on Barrett’s esophagus. https://pubmed.ncbi.nlm.nih.gov/29122929/
- Reid BJ, Li X, Galipeau PC, Vaughan TL. Barrett’s esophagus and esophageal adenocarcinoma. https://pubmed.ncbi.nlm.nih.gov/20094044/
- Sharma P, Katzka D, Gupta N. Barrett’s esophagus: Epidemiology, clinical manifestations, and diagnosis. https://pubmed.ncbi.nlm.nih.gov/31335037/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge