Pterygium: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Pterygium is a common ocular surface disorder characterized by a triangular fibrovascular proliferation of conjunctival tissue extending onto the cornea. It is strongly associated with chronic ultraviolet (UV) radiation exposure, environmental irritants, and ocular surface inflammation. While early lesions may remain asymptomatic, progressive pterygium can induce astigmatism, visual impairment, and cosmetic concerns.
We report the case of a 48-year-old male presenting with chronic ocular irritation, redness, and progressive visual blurring in the right eye. Clinical examination and anterior segment imaging confirmed the diagnosis of primary nasal pterygium. Surgical excision with conjunctival autograft was performed, resulting in excellent visual and cosmetic outcomes with no recurrence at 3-month follow-up.
This case underscores the importance of early recognition, risk factor modification, and appropriate surgical intervention in managing pterygium and preventing recurrence.
Introduction
Pterygium is a degenerative and hyperplastic condition of the ocular surface involving fibrovascular tissue proliferation from the bulbar conjunctiva onto the cornea. It is particularly prevalent in populations residing in equatorial and tropical regions, often referred to as the “pterygium belt,” where UV exposure is high.
The pathogenesis is multifactorial and involves:
• Chronic ultraviolet-B (UV-B) radiation–induced damage
• Limbal stem cell deficiency
• Activation of fibroblasts and angiogenic pathways
• Chronic inflammation and extracellular matrix remodeling
Thiamine-like oxidative stress mechanisms and p53 gene mutations have also been implicated in disease progression.
Major risk factors include:
• Prolonged outdoor exposure (e.g., farmers, construction workers)
• Dry, dusty, and windy environments
• Chronic ocular surface irritation
• Lack of protective eyewear
Clinically, pterygium appears as a triangular fibrovascular growth, most commonly arising from the nasal conjunctiva. It may remain stationary or progressively invade the cornea.
Common clinical manifestations include:
• Redness and irritation
• Foreign body sensation
• Dryness and burning
• Visual disturbance due to induced astigmatism or axis involvement
This case report highlights the clinical presentation, diagnostic workup, and management of pterygium, emphasizing surgical intervention and preventive strategies.
Case Report
Patient History
A 48-year-old male presented to the ophthalmology outpatient department with complaints of:
• Persistent redness in the right eye for 6 months
• Foreign body sensation and intermittent irritation
• Gradual blurring of vision over the past 2 months
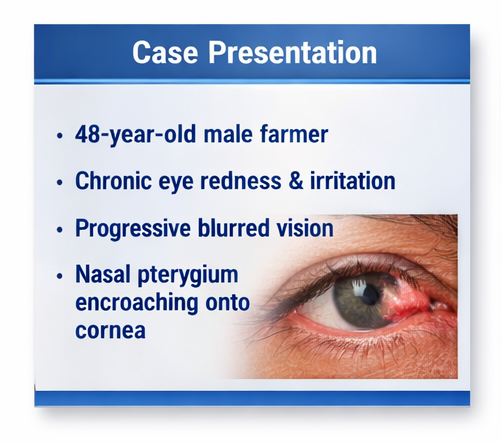
The patient had a significant occupational history as a farmer, with prolonged daily exposure to sunlight, dust, and wind. He reported inconsistent use of protective eyewear. There was no history of ocular trauma, prior surgery, or contact lens use.
Past medical history was unremarkable, and there were no systemic comorbidities such as diabetes or hypertension.
Clinical Examination
On ophthalmic evaluation:
• Visual acuity: 6/9 in the right eye and 6/6 in the left eye
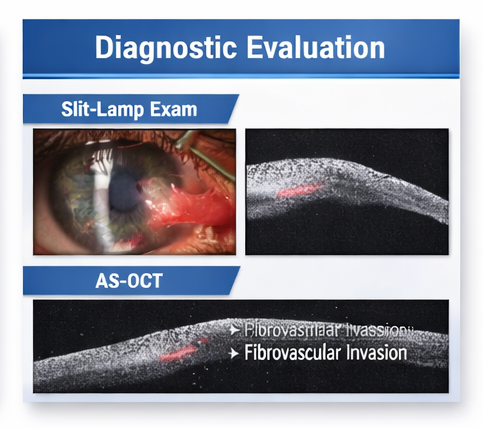
• Slit-lamp examination revealed a fleshy, triangular fibrovascular growth extending from the nasal conjunctiva onto the cornea
• The lesion extended approximately 2.5–3 mm beyond the limbus
• Mild conjunctival hyperemia and tear film instability were noted
Corneal involvement resulted in mild surface irregularity contributing to astigmatism. The anterior chamber and fundus examination were normal.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Pterygium
• Pinguecula (non-invasive conjunctival degeneration)
• Ocular surface squamous neoplasia (OSSN)
• Chronic conjunctivitis
• Limbal dermoid
The progressive corneal encroachment and fibrovascular characteristics favored a diagnosis of pterygium.
Investigations
Ophthalmic Assessment
• Keratometry showed with-the-rule astigmatism in the affected eye
• Tear break-up time (TBUT) was reduced, indicating associated dry eye
Imaging
Anterior segment optical coherence tomography (AS-OCT) demonstrated:
• Hyperreflective subepithelial fibrovascular tissue
• Disruption of Bowman’s membrane
• Superficial corneal invasion
These findings supported the diagnosis and helped assess lesion depth.
Diagnosis
Based on clinical findings and imaging, a diagnosis of primary progressive nasal pterygium of the right eye was established.
Management and Outcome
Management Strategy
Initial Medical Management
• Preservative-free lubricating eye drops
• UV-protective sunglasses advised
• Short course of topical non-steroidal anti-inflammatory agents
Due to progressive symptoms and visual impact, surgical intervention was indicated.
Surgical Treatment
The patient underwent:
• Pterygium excision
• Conjunctival autograft transplantation
• Fibrin glue fixation
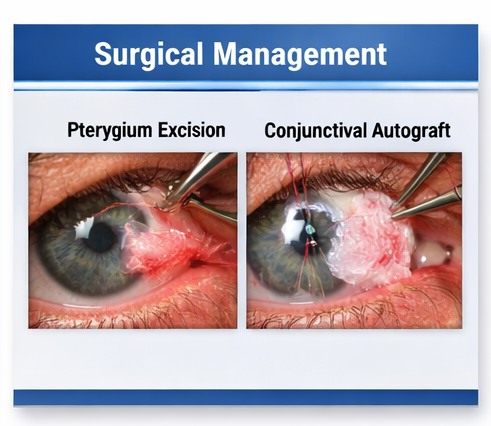
This technique is considered the gold standard due to its lower recurrence rates compared to bare sclera excision.
Postoperative Care
• Topical antibiotic-steroid combination drops
• Lubricants for ocular surface stabilization
• Patient education on sun protection and eye care
Follow-Up and Outcome
At 1 week:
• Mild postoperative inflammation
• Graft intact and well-positioned
At 4 weeks:
• Significant reduction in redness and irritation
• Visual acuity improved to 6/6
At 8 weeks:
• Stable ocular surface
• No signs of recurrence
At 12 weeks:
• Complete recovery with excellent cosmetic outcome
• No complications or graft-related issues
Discussion
Pathophysiology
Pterygium development is driven by UV-induced oxidative stress leading to:
• DNA damage and abnormal cell proliferation
• Activation of matrix metalloproteinases (MMPs)
• Angiogenesis mediated by vascular endothelial growth factor (VEGF)
• Breakdown of corneal stromal architecture
Limbal stem cell deficiency plays a central role, allowing conjunctival tissue to invade the cornea.
Diagnostic Challenges
Diagnosis is primarily clinical; however, challenges arise in distinguishing pterygium from premalignant lesions such as OSSN.
Key diagnostic tools include:
• Slit-lamp biomicroscopy
• AS-OCT imaging
• Histopathological examination (if atypical features present)
Early-stage pterygium may resemble pinguecula, which lacks corneal invasion.
Treatment Considerations
Conservative Management
Indicated for mild, asymptomatic cases:
• Lubricants
• Anti-inflammatory drops
• UV protection
Surgical Management
Indications include:
• Visual impairment
• Progressive growth
• Induced astigmatism
• Cosmetic concerns
Conjunctival autografting remains the preferred technique due to:
• Lower recurrence rates (5–15%)
• Better cosmetic outcomes
• Restoration of limbal barrier
Adjunctive therapies such as mitomycin-C may be used in recurrent cases but require caution due to potential complications.
Complications
Potential complications include:
• Recurrence (most common)
• Graft displacement or edema
• Infection
• Scleral thinning (rare)
Recurrence is influenced by surgical technique, patient compliance, and continued UV exposure.
Prognosis
The prognosis of pterygium is generally favorable with appropriate management.
Factors influencing outcomes include:
• Surgical expertise
• Postoperative care adherence
• Environmental exposure control
Early surgical intervention in progressive cases results in excellent functional and cosmetic outcomes, as demonstrated in this case.
Conclusion
Pterygium is a common ocular surface disorder with the potential to cause significant visual morbidity if left untreated. This case highlights the importance of early diagnosis, identification of risk factors, and timely surgical intervention.
Conjunctival autograft remains the gold standard surgical approach, offering low recurrence rates and favorable outcomes. Preventive strategies, including UV protection and patient education, are essential in reducing disease burden and recurrence risk.
Clinician awareness and proactive management are critical in ensuring optimal patient outcomes in pterygium.
References
- Ang LP, Chua JL, Tan DT. Pterygium: epidemiology, pathogenesis, and treatment. Survey of Ophthalmology. https://pubmed.ncbi.nlm.nih.gov/17363000/
- StatPearls. Pterygium. National Center for Biotechnology Information. https://www.ncbi.nlm.nih.gov/books/NBK558907/
- Clearfield E, Muthappan V, Wang X, Kuo IC. Conjunctival autograft for pterygium. Cochrane Database. https://pubmed.ncbi.nlm.nih.gov/26867412/
- Coroneo MT. Pterygium as an early indicator of ultraviolet insolation. British Journal of Ophthalmology. https://bjo.bmj.com/content/75/11/689
- Moran DJ, Hollows FC. Pterygium and ultraviolet radiation. https://pubmed.ncbi.nlm.nih.gov/6731531/
- American Academy of Ophthalmology. Pterygium Preferred Practice Pattern. https://www.aao.org/preferred-practice-pattern/pterygium-ppp
- Hirst LW. The treatment of pterygium. Survey of Ophthalmology. https://pubmed.ncbi.nlm.nih.gov/19168249/
- Tan DT, Chee SP, Dear KB, Lim AS. Effect of pterygium morphology on recurrence. Ophthalmology. https://pubmed.ncbi.nlm.nih.gov/9331205/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge