Congenital Heart Disease In Children
All SpecialityPage Navigation
ABSTRACT
Congenital heart disease (CHD) is the most common congenital disorder in neonates.
A number of factors including genetic factors, teratogenic exposure and several other unrecognised factors have been associated with its development.
Ventricular Septal Defect (VSD) is the most common type.
INTRODUCTION-
Congenital Heart Defects are structural abnormalities of heart and/or great blood vessels during fetal development.
CHDs account for about 28% of all congenital anomalies. It is a result of lack of normal development of heart during the embryonic phase.
Prevalence- 1% births in the United States.
1.5-1.7/1000 live births in India.
ETIOLOGY –
Mostly unknown.
Sometimes associated with –
• Chromosomal abnormalities and Genetic disorders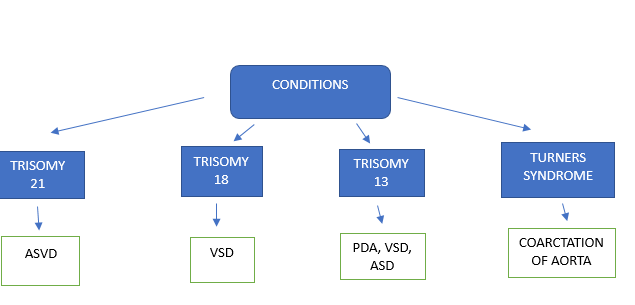
• Teratogenic factors including maternal smoking, alcohol abuse, exposure to retinoid, indomethacin, tocolytics.
• Maternal infection with rubella.
• Additionally, history of epilepsy in mother, phenylketonuria, maternal age above 30, Type 1 and Type 2 DM as well as positive family history are other risk factors.
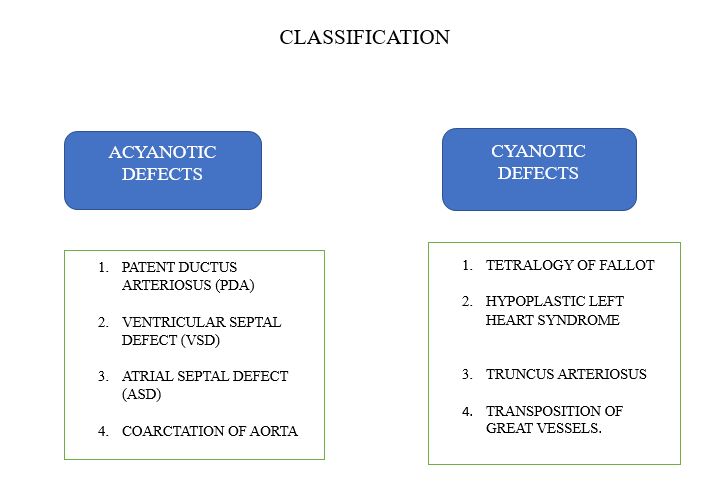
ASD –
• Abnormal opening in the septum between right and left atrium.
• Normally L to R shunt.
• Most common type is secundum ASD (80%).
• Wide fixed split s2 is the pathognomic for ASD.
• Clinical manifestations are non-specific.
VSD –
• Defect in interventricular septum.
• Shunting of blood from L to R.
• Most common type is peri membranous.
• Holosystolic/ high pitched murmur
• Small VSDs are usually asymptomatic. Moderate VSDs can cause frequent respiratory infections and fatigue.
• Larger VSD can lead to reversal of shunt in Eisenmenger syndrome.
TETRAOGY OF FALLOT –
• 4 Defects are present in the heart
1) Right ventricular outflow obstruction
2) Right ventricular hypertrophy
3) Overriding aorta
4) Ventricular septal defect
• Clinical manifestations include cyanosis, tachypnoea, “tet spells”
• Harsh systolic ejection murmur (best heard at left sternal border)
• Boot shaped heart on CXR.
• Surgical repair definitive
COARCTATION OF AORTA –
• Narrowing of the descending aorta typically located at the insertion point of the ductus arteriosus, just distal to the left subclavian artery
• Often associated with bicuspid aortic valve and turners syndrome
• Posterior rib notching and figure 3 sign on CXR.
PATENT DUCTUS ARTERIOSUS –
• Condition in which ductus arteriosus (small artery which connects fetal pulmonary artery to aorta) remains patent and does not close after birth.
• Epidemiology –
1. Prematurity
2. 2:1 female predominance
3. Higher altitude
4. Congenital rubella
• Caused from continual prostaglandin E1 production
• Continuous machine-like murmur and bounding peripheral pulses on physical exam.
PREVENTION –
Prevention of congenital anomalies is important as the impact can be for life. Environmental factors known to be the risk factors in etiology need to be suitably addressed. First approach should be for families with children or relatives with CHD. Second, environmental factors need to be suitably addressed.
DETECTION AND DIAGNOSIS-
Early detection is desirable. The suspicion of CHD is mainly clinical. Evaluation should be done on the basis of Nadas’ criteria for diagnosis of CHD.
The major criteria include -
1. Systolic murmur grade 3 or more
2. Diastolic murmur
3. Cyanosis
4. Congestive cardiac failure
The minor criteria include –
1. Abnormal echo
2. Abnormal X ray
3. Abnormal BP
Presence of 1 major or 2 minor criteria indicates heart disease.
In infants, feeding difficulties are common. Others include poor weight gain, irritability, breathing difficulty, inappropriate sweating and persistent cough.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge