Optic Neuritis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Optic neuritis is an acute inflammatory demyelinating disorder of the optic nerve that commonly presents with sudden visual loss, ocular pain, and impaired color vision. It is frequently associated with multiple sclerosis (MS) and other autoimmune or infectious conditions. Early diagnosis and prompt treatment are important to preserve visual function and reduce long-term neurological complications.
We present the case of a 32-year-old female who presented with acute unilateral visual loss associated with pain during eye movement and reduced color perception. Ophthalmological examination, magnetic resonance imaging (MRI), visual evoked potentials, and laboratory investigations confirmed the diagnosis of demyelinating optic neuritis. The patient was managed with intravenous corticosteroid therapy followed by oral steroids and neurological follow-up, resulting in marked visual improvement.
This case highlights the importance of early recognition, neuro-ophthalmic evaluation, and multidisciplinary management in patients with optic neuritis to improve visual and neurological outcomes.
Introduction
Optic neuritis is an inflammatory disorder involving the optic nerve and is characterized by acute or subacute visual impairment. The condition most commonly affects young adults, especially females between 20–45 years of age. It is considered one of the most frequent causes of sudden visual loss in young individuals.
Optic neuritis is commonly associated with demyelinating disorders such as multiple sclerosis, neuromyelitis optica spectrum disorder (NMOSD), and myelin oligodendrocyte glycoprotein antibody-associated disease (MOGAD). Infectious, autoimmune, and inflammatory causes may also contribute.
The pathophysiology involves inflammatory demyelination of the optic nerve, leading to impaired conduction of visual signals from the retina to the brain.
Important risk factors and associations include:
• Multiple sclerosis
• Autoimmune diseases
• Viral infections
• Female gender
• Genetic susceptibility
• Neuromyelitis optica
• MOG antibody disease
• Systemic inflammatory disorders
Common clinical manifestations include:
• Sudden visual loss
• Pain during eye movement
• Reduced color vision
• Blurred vision
• Visual field defects
• Reduced contrast sensitivity
• Relative afferent pupillary defect (RAPD)
Early diagnosis and treatment are important to reduce visual disability and identify associated neurological disorders.
Case Report
Patient History
A 32-year-old female presented to the ophthalmology outpatient department with:
• Sudden painless blurring of vision in the right eye for 5 days
• Pain during eye movement
• Difficulty identifying colors
• Reduced central vision
• Mild frontal headache
The patient reported progressive worsening of vision over 3 days. There was no history of ocular trauma or previous ophthalmological surgery.
Past medical history revealed:
• Intermittent tingling sensation in lower limbs 1 year earlier
• No diabetes mellitus
• No hypertension
• No tuberculosis
• No known autoimmune disease
There was no family history of hereditary ocular disorders.
Clinical Examination
General Examination
• Afebrile
• Pulse rate: 78/min
• Blood pressure: 118/76 mmHg
• Systemically stable
Ophthalmological Examination
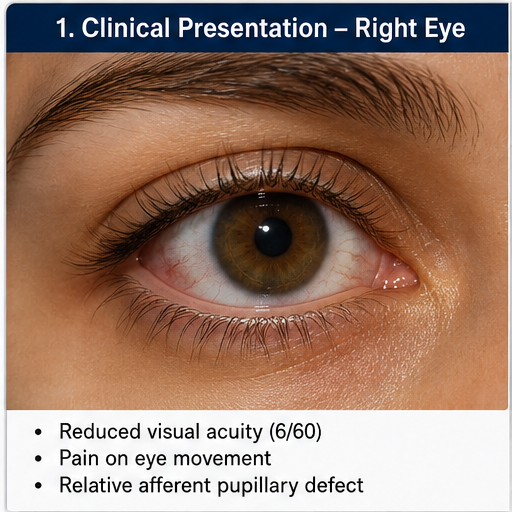
Visual acuity:
• Right eye: 6/60
• Left eye: 6/6
Other findings included:
• Reduced color vision in right eye
• Pain on extraocular movement
• Relative afferent pupillary defect in right eye
• Mild optic disc edema
• Impaired contrast sensitivity
• Central scotoma on visual field examination
Fundus examination of the left eye was normal.
Neurological examination showed no major focal neurological deficits.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Optic neuritis
• Ischemic optic neuropathy
• Compressive optic neuropathy
• Retinal vascular occlusion
• Neuromyelitis optica
• Intracranial space-occupying lesion
• Functional visual loss
The acute visual loss associated with pain during eye movement and color vision impairment strongly suggested optic neuritis.
Investigations
Laboratory Findings
• Complete blood count: Normal
• ESR and CRP: Mildly elevated
• Blood glucose: Normal
• ANA profile: Negative
• Aquaporin-4 antibody: Negative
• MOG antibody: Negative
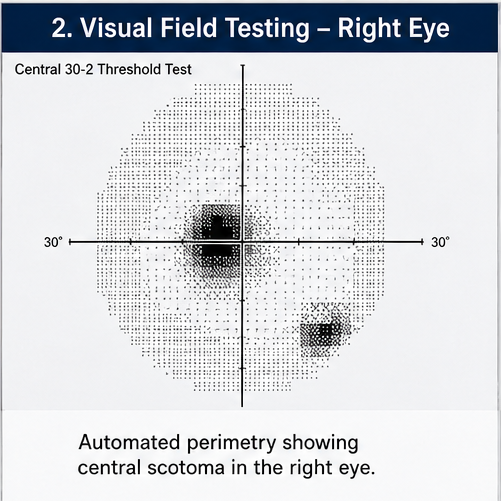
Visual Field Testing
Automated perimetry revealed:
• Central scotoma in the right eye
• Reduced visual sensitivity
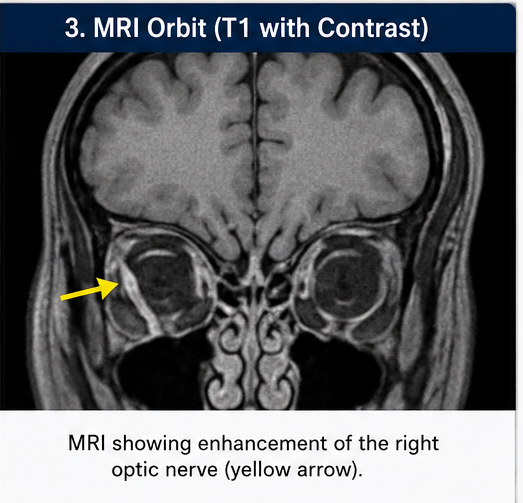
Magnetic Resonance Imaging (MRI)
MRI brain and orbit revealed:
• Enhancement of the right optic nerve
• T2 hyperintense demyelinating lesions
• Periventricular white matter plaques suggestive of demyelination
These findings supported a diagnosis of demyelinating optic neuritis associated with possible early multiple sclerosis.
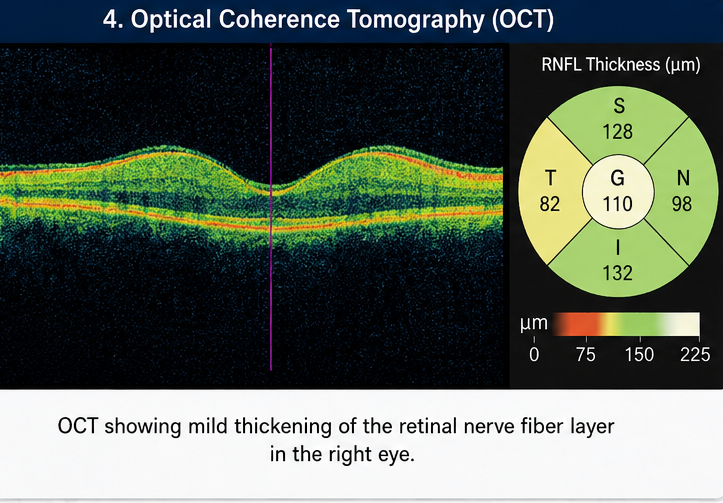
Optical Coherence Tomography (OCT)
OCT demonstrated:
• Mild retinal nerve fiber layer swelling
• Optic nerve inflammation
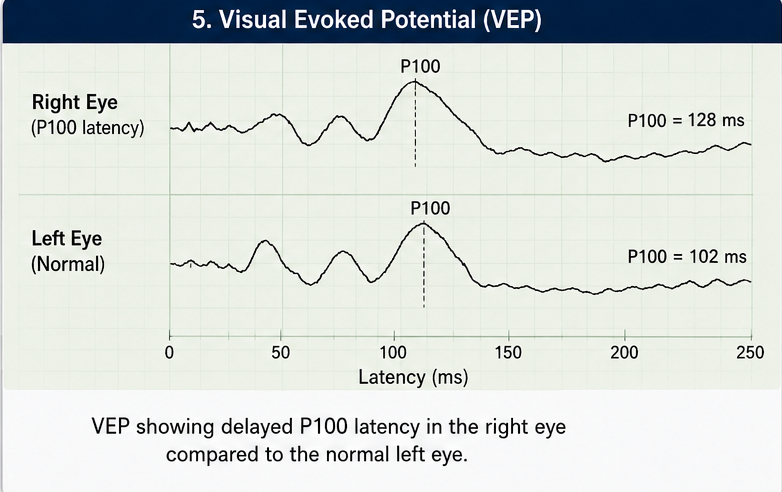
Visual Evoked Potential (VEP)
VEP showed:
• Delayed P100 latency
• Reduced conduction along the optic nerve
Diagnosis
Based on clinical presentation, ophthalmological findings, MRI evaluation, and electrophysiological studies, a diagnosis of Acute Demyelinating Optic Neuritis was established.
Management and Outcome
Initial Management
The patient was counseled regarding:
• Nature of the disease
• Possibility of recurrence
• Association with multiple sclerosis
• Need for neurological follow-up
• Importance of treatment adherence
Medical Management
The patient received:
• Intravenous methylprednisolone 1 g/day for 3 days
• Oral prednisolone taper therapy
• Vitamin supplementation
• Lubricating eye drops
• Neuroprotective supportive care
Neurological Monitoring
The patient was referred for neurological evaluation to assess the risk of multiple sclerosis progression.
Follow-Up and Clinical Course
At 1 Week
• Reduced ocular pain
• Mild improvement in vision
• Improved color perception
At 1 Month
• Visual acuity improved to 6/18
• Significant reduction in visual blurring
• Improved daily functioning
At 3 Months
• Visual acuity improved to 6/9
• No recurrence of symptoms
• Stable neurological status
At 6 Months
• Stable visual recovery
• No new neurological deficits
• Continued MRI surveillance advised
The patient remained under regular ophthalmology and neurology follow-up.
Discussion
Pathophysiology
Optic neuritis primarily results from inflammatory demyelination of the optic nerve. The inflammatory process damages the myelin sheath surrounding optic nerve fibers, leading to impaired neural conduction and visual dysfunction.
Important pathological mechanisms include:
• Immune-mediated demyelination
• T-cell activation
• Axonal injury
• Cytokine-mediated inflammation
• Blood-brain barrier disruption
• Neurodegeneration
The inflammatory response may occur as an isolated event or as part of systemic demyelinating disease.
Epidemiology
Important epidemiological features include:
• Commonly affects young adults
• Female predominance
• Frequently associated with multiple sclerosis
• Annual incidence approximately 1–5 per 100,000 population
• Often unilateral at presentation
Optic neuritis remains an important early neurological manifestation of demyelinating disease.
Clinical Manifestations
Common manifestations include:
• Acute visual loss
• Ocular pain
• Reduced color vision
• Central visual field defects
• Reduced contrast sensitivity
• Photopsia
• Relative afferent pupillary defect
Some patients may additionally develop:
• Bilateral visual involvement
• Recurrence
• Neurological symptoms suggestive of multiple sclerosis
Diagnostic Considerations
Important diagnostic modalities include:
- Detailed ophthalmological examination
- Visual acuity assessment
- Visual field testing
- Optical coherence tomography
- Visual evoked potential
- MRI brain and orbit
- Autoimmune antibody testing
MRI plays an important role in identifying demyelinating lesions and predicting future risk of multiple sclerosis.
Treatment Modalities
Conservative Management
Supportive measures include:
• Visual rest
• Psychological reassurance
• Neurological monitoring
• Patient education
Pharmacological Therapy
Medical treatment options include:
• Intravenous corticosteroids
• Oral corticosteroid taper
• Immunomodulatory therapy
• Disease-modifying therapy in MS-associated cases
Long-Term Monitoring
Patients require monitoring for:
• Visual recovery
• Recurrence
• Development of multiple sclerosis
• Neurological complications
Complications
Potential complications include:
• Persistent visual impairment
• Reduced color vision
• Optic nerve atrophy
• Recurrence of optic neuritis
• Multiple sclerosis progression
• Psychological stress
• Reduced quality of life
Delayed diagnosis may result in permanent optic nerve damage.
Prognosis
The prognosis depends upon:
• Severity of inflammation
• Early initiation of therapy
• Underlying neurological disease
• MRI lesion burden
• Recurrence risk
• Long-term neurological follow-up
Most patients experience partial or substantial visual recovery within several weeks to months.
Conclusion
Optic neuritis is an important inflammatory demyelinating disorder that may represent the first clinical manifestation of multiple sclerosis or related neurological diseases. Sudden visual loss, pain during eye movement, and impaired color vision should prompt immediate ophthalmological and neurological evaluation.
This case highlights the importance of MRI evaluation, electrophysiological studies, corticosteroid therapy, and long-term neurological monitoring in achieving favorable visual outcomes. Early multidisciplinary management and regular follow-up remain essential for reducing visual disability and identifying future neurological progression.
References
- Optic Neuritis Study Group. Multiple sclerosis risk after optic neuritis. https://pubmed.ncbi.nlm.nih.gov/11502909/
- Balcer LJ. Clinical practice. Optic neuritis. https://pubmed.ncbi.nlm.nih.gov/17229952/
- Toosy AT, Mason DF, Miller DH. Optic neuritis. https://pubmed.ncbi.nlm.nih.gov/17382830/
- Petzold A, Wattjes MP, Costello F, et al. The investigation of acute optic neuritis. https://pubmed.ncbi.nlm.nih.gov/28596234/
- Bennett JL. Optic neuritis. https://pubmed.ncbi.nlm.nih.gov/24656272/
- National Eye Institute. Optic Neuritis. https://www.nei.nih.gov/learn-about-eye-health/eye-conditions-and-diseases/optic-neuritis
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Efficacy and safety of intravenous chemotherapy in children with intraocular retinoblastoma
2.
Certain Oral Bacteria May Be a Risk Factor for Head and Neck Cancer
3.
Quads, Frailty, and the Future: Evolving Frontline Strategies in Multiple Myeloma
4.
Top Cancer Centers; Phase III Win in Prostate Cancer; Screening Recs for Anal Cancer
5.
Traveling to Die: The Latest Form of Medical Tourism
1.
HPV and Immunotherapy in Cancer Survivorship: National Cancer Survivors Day Review
2.
Unlocking the Immune Arsenal: A Revolution in Cancer Treatment
3.
Polycythemia Vera: A Historical Perspective and Contemporary Management
4.
The Benefits and Risks of Transurethral Resection of Bladder Tumor
5.
Colon cancer: Risk factors, warning signs and treatment options
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Experts' Opinion on the Goal of Treatment of Patients with Relapsed Adult B-cell ALL
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Blood Cancer- Further Discussion on Genomic Testing & Advancement in Diagnosis and Treatment
4.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part VII
5.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge