Hyperemesis Gravidarum During Pregnancy: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Hyperemesis gravidarum is a severe and potentially life-threatening form of nausea and vomiting during pregnancy, characterized by persistent vomiting, dehydration, electrolyte imbalance, ketonuria, and significant weight loss. It represents the extreme end of the spectrum of pregnancy-related nausea and vomiting and can lead to serious maternal and fetal complications if not managed appropriately. The etiology is multifactorial, involving hormonal, genetic, and psychological components. Early recognition and prompt intervention are essential to prevent adverse outcomes. This case report describes a 26-year-old primigravida presenting with severe hyperemesis gravidarum in early pregnancy. It highlights the clinical presentation, diagnostic workup, therapeutic management, and favorable maternal and fetal outcomes following timely treatment.
Introduction
Hyperemesis gravidarum is a clinical condition defined by severe, intractable nausea and vomiting during pregnancy that results in dehydration, electrolyte imbalance, ketosis, and weight loss exceeding 5% of pre-pregnancy body weight. It typically manifests during the first trimester, most commonly between 6 and 12 weeks of gestation, and may persist into the second trimester in some patients.
The exact pathophysiology remains incompletely understood, but elevated levels of human chorionic gonadotropin (hCG) and estrogen are considered major contributors. Additional factors such as gastrointestinal dysmotility, genetic susceptibility, and psychosocial influences may also play a role. Unlike normal pregnancy-related nausea, hyperemesis gravidarum is associated with systemic complications including renal dysfunction, hepatic abnormalities, nutritional deficiencies, and neurological complications such as Wernicke’s encephalopathy.
Given its potential severity, early diagnosis and appropriate management are critical to reduce maternal morbidity and ensure optimal fetal outcomes.
Case Report
Patient History
A 26-year-old primigravida at 9 weeks of gestation presented to the obstetrics department with complaints of persistent nausea and severe vomiting for the past 3 weeks. The vomiting frequency had progressively increased, reaching up to 8–10 episodes per day, and was not relieved by dietary modifications.
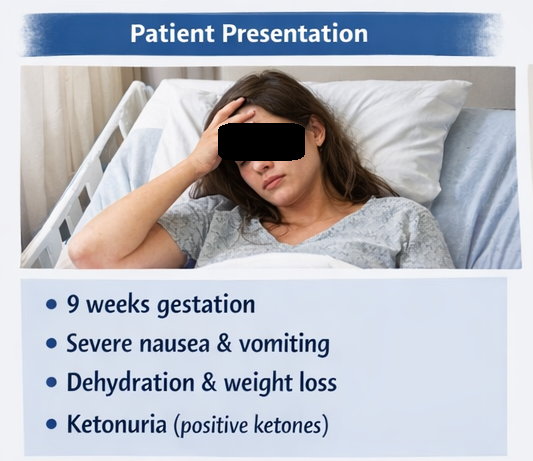
The patient reported inability to tolerate oral intake, significant fatigue, dizziness, and decreased urine output. She also noted a weight loss of approximately 4 kilograms over a 2-week period. There was no history of abdominal pain, fever, diarrhea, or urinary symptoms.
Her past medical history was unremarkable, and she had no history of thyroid disease or gastrointestinal disorders. There was no history of similar symptoms in previous pregnancies, as this was her first pregnancy. She was not on any chronic medications.
Clinical Examination
General Examination
- Ill-looking and dehydrated
- Dry mucous membranes
- Sunken eyes
- Decreased skin turgor
Vital Signs
- Blood pressure: 90/60 mmHg
- Pulse rate: 104/min (tachycardia)
- Respiratory rate: Normal
- Temperature: Afebrile
Abdominal Examination
- Soft and non-tender
- No guarding or rigidity
- No hepatosplenomegaly
Clinical Evaluation
Differential Diagnosis
- Hyperemesis gravidarum
- Acute gastroenteritis
- Urinary tract infection
- Molar pregnancy
- Thyrotoxicosis
The presence of persistent vomiting, dehydration, ketonuria, and significant weight loss strongly suggested hyperemesis gravidarum.
Investigations
Laboratory Findings
- Complete Blood Count (CBC)
- Elevated hematocrit indicating hemoconcentration
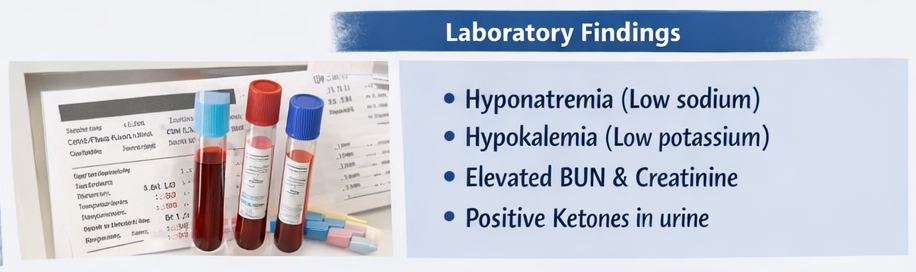
- Serum Electrolytes
- Hyponatremia (low sodium)
- Hypokalemia (low potassium)
- Renal Function Tests
- Mild elevation in blood urea nitrogen and creatinine
- Urinalysis
- Positive for ketones (ketonuria)
- Liver Function Tests
- Mildly elevated transaminases
- Thyroid Function Tests
- Within normal limits
Imaging
Ultrasound Abdomen and Pelvis
- Single viable intrauterine pregnancy at 9 weeks gestation
- No evidence of molar pregnancy or multiple gestation
Diagnosis
Severe hyperemesis gravidarum with dehydration, electrolyte imbalance, and ketosis
Management and Outcome
Treatment Plan
Hospital Admission
- Patient admitted for stabilization and close monitoring

Fluid and Electrolyte Management
- Intravenous normal saline infusion
- Potassium supplementation to correct hypokalemia
Pharmacological Therapy
- Antiemetics: ondansetron and metoclopramide
- Vitamin supplementation: pyridoxine (vitamin B6) and thiamine to prevent neurological complications
Nutritional Support
- Gradual reintroduction of oral intake
- Small, frequent, high-protein meals
Follow-Up and Clinical Progress
After 72 Hours
- Significant reduction in vomiting episodes
- Improved hydration status
- Normalization of electrolyte levels
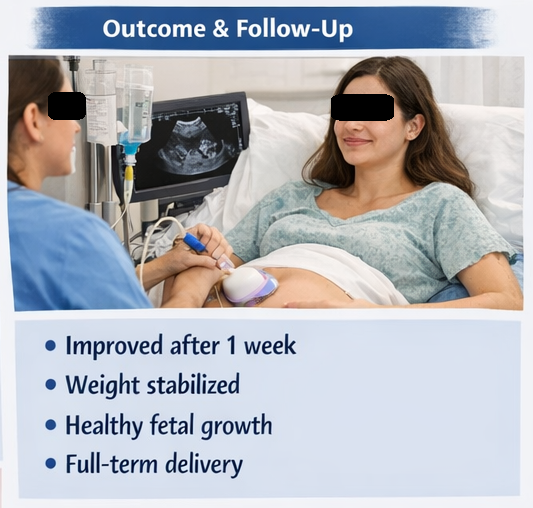
At 1 Week
- Patient able to tolerate oral feeds
- Discharged on oral antiemetics and dietary advice
At 4 Weeks Follow-Up
- Weight stabilized
- No recurrence of severe vomiting
- Normal fetal growth confirmed on ultrasound
Second Trimester
- Complete resolution of symptoms
The remainder of the pregnancy was uneventful, and the patient delivered a healthy full-term infant.
Discussion
Hyperemesis gravidarum is a severe form of pregnancy-related nausea and vomiting that goes beyond typical morning sickness and can lead to significant maternal complications if untreated. It is characterized by persistent vomiting, dehydration, electrolyte imbalance, ketosis, and nutritional deficiencies, affecting multiple organ systems. Due to its severity, it is one of the most common causes of hospitalization in early pregnancy, often requiring intravenous fluids, electrolyte correction, and antiemetic therapy.
The condition also has a notable impact on quality of life, contributing to fatigue, psychological distress, and reduced daily functioning. Its pathophysiology is multifactorial, with hormonal factors such as elevated human chorionic gonadotropin (hCG) and estrogen playing a key role, along with possible genetic and gastrointestinal influences. Early recognition and timely management are essential to prevent complications such as renal dysfunction, Wernicke’s encephalopathy, and adverse fetal outcomes.
Pathophysiology
The pathogenesis is multifactorial:
- Elevated hCG levels stimulate the central vomiting center
- Increased estrogen levels impair gastric motility
- Altered gastrointestinal function contributes to nausea
- Psychological and genetic factors may influence susceptibility
Risk Factors
- First pregnancy (primigravida)
- Multiple gestation
- Previous history of hyperemesis
- Obesity
- Molar pregnancy
Clinical Features
- Persistent nausea and vomiting
- Dehydration
- Weight loss exceeding 5%
- Ketonuria
- Electrolyte imbalance
- Weakness and dizziness
Diagnostic Approach
Step 1: Confirmation of Severity
- Presence of dehydration
- Electrolyte imbalance
- Ketonuria
Step 2: Exclusion of Other Causes
- Thyroid disorders
- Gastrointestinal infections
- Molar pregnancy (via ultrasound)
Management Strategies
Supportive Therapy
- Intravenous fluids
- Electrolyte correction
Pharmacological Treatment
- Antiemetics (ondansetron, metoclopramide)
- Vitamin B6 and thiamine
Nutritional Therapy
- Small frequent meals
- High-protein diet
Advanced Care
- Enteral or parenteral nutrition in refractory cases
Complications
Maternal
- Severe dehydration
- Electrolyte imbalance
- Wernicke’s encephalopathy
- Acute kidney injury
Fetal
- Low birth weight
- Preterm delivery
Prognosis
- Excellent with early diagnosis and treatment
- Most cases resolve by mid-pregnancy
- Recurrence risk in future pregnancies
Conclusion
Hyperemesis gravidarum is a serious but manageable condition when identified early. This case highlights the importance of recognizing key clinical features such as persistent vomiting, dehydration, and weight loss, followed by appropriate diagnostic evaluation.
Timely intervention with fluid resuscitation, antiemetics, and nutritional support can lead to rapid clinical improvement and prevent complications. A multidisciplinary approach involving obstetricians and physicians is essential to ensure optimal maternal and fetal outcomes.
References
- Niebyl JR. Nausea and vomiting in pregnancy. https://pubmed.ncbi.nlm.nih.gov/16034031/
- Verberg MF, et al. Hyperemesis gravidarum: a literature review. https://pubmed.ncbi.nlm.nih.gov/18508982/
- Bailit JL. Hyperemesis gravidarum: epidemiologic findings. https://pubmed.ncbi.nlm.nih.gov/15051562/
- Goodwin TM. Hyperemesis gravidarum. https://pubmed.ncbi.nlm.nih.gov/10819852/
- Chiossi G, et al. Wernicke encephalopathy in hyperemesis gravidarum. https://pubmed.ncbi.nlm.nih.gov/20502331/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge