Renal Atresia: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Renal atresia is a rare congenital anomaly characterized by the absence or complete closure of a segment of the renal collecting system or ureter, resulting in impaired urinary drainage and progressive renal dysfunction. It may present in isolation or as part of complex urogenital malformations. Clinical manifestations vary depending on the extent of obstruction and whether the condition is unilateral or bilateral, ranging from asymptomatic cases to severe renal impairment.
We present the case of a 3-year-old child diagnosed with unilateral renal atresia following recurrent urinary tract infections and abdominal discomfort. Imaging studies revealed absence of a functional ureteral lumen on the affected side, leading to progressive hydronephrosis and renal dysplasia. Early surgical intervention and long-term follow-up resulted in stabilization of renal function and prevention of further complications.
This case highlights the importance of early detection, appropriate imaging, and timely management in improving outcomes in patients with renal atresia.
Introduction
Renal atresia is a congenital malformation involving the developmental failure of a segment of the urinary tract, most commonly affecting the ureter or renal pelvis. This results in obstruction of urine flow, leading to backpressure changes such as hydronephrosis, renal parenchymal damage, and eventual loss of renal function.
The condition is often detected prenatally through ultrasonography or postnatally when patients present with recurrent urinary tract infections, abdominal mass, or impaired renal function. Renal atresia may occur as an isolated defect or in association with other congenital anomalies such as vesicoureteral reflux or multicystic dysplastic kidney.
Advancements in prenatal imaging, ultrasonography, and nuclear renal scans have significantly improved early diagnosis and management strategies. Treatment is guided by the severity of obstruction, renal function, and presence of complications.
Case Report
Patient History
A 3-year-old male child was brought to the pediatric outpatient department with complaints of recurrent fever, irritability, and episodes of abdominal pain over the past six months. The parents reported multiple episodes of urinary tract infections treated with antibiotics at local clinics.
There was no history of hematuria or urinary incontinence. The child was born full-term via normal vaginal delivery with no significant antenatal complications. No prenatal anomaly scan abnormalities were reported.
Family history was unremarkable for renal or congenital anomalies.
Clinical Examination
General Examination
The child was moderately built and nourished. Vital signs were stable, with a mild elevation in temperature (38°C). No pallor, edema, or signs of systemic illness were noted.
Abdominal Examination
Palpation revealed a vague, non-tender mass in the left flank region. There was no guarding or rigidity.
Systemic Examination
Other systems were within normal limits.
Clinical Evaluation
Differential Diagnosis
Based on the presenting symptoms and physical findings, the following conditions were considered:
- Hydronephrosis due to ureteropelvic junction obstruction
- Vesicoureteral reflux
- Multicystic dysplastic kidney
- Renal atresia
- Obstructive uropathy secondary to congenital anomalies
The recurrent infections and palpable mass raised suspicion of an underlying obstructive pathology.
Investigations
Imaging Studies
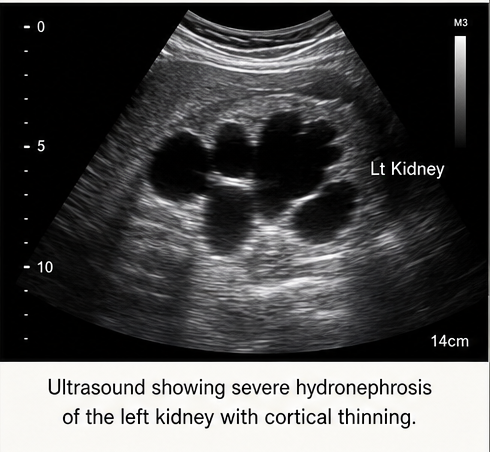
Ultrasonography (USG):
Revealed significant hydronephrosis of the left kidney with cortical thinning. The ureter was not clearly visualized.
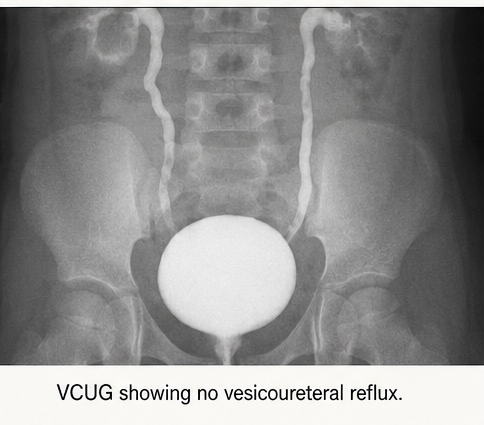
Voiding Cystourethrogram (VCUG):
Showed no evidence of vesicoureteral reflux.
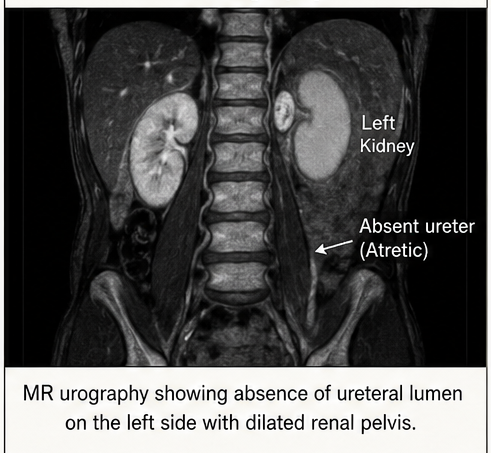
Magnetic Resonance Urography (MRU):
Demonstrated absence of a patent ureteral lumen on the left side, consistent with ureteral atresia. The left kidney appeared dysplastic with reduced functional tissue.
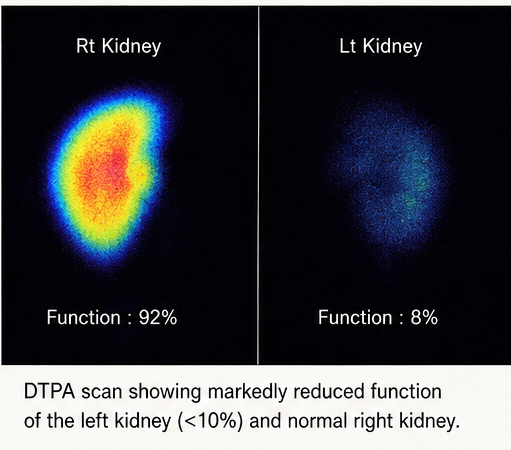
Renal Nuclear Scan (DTPA Scan):
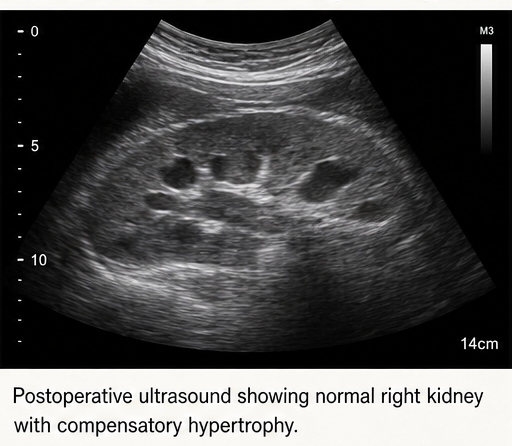
Indicated markedly reduced function in the left kidney (<10%), while the right kidney showed compensatory hypertrophy with normal function.
Laboratory Investigations
- Complete blood count: Mild leukocytosis
- Serum creatinine: Within normal range
- Blood urea nitrogen: Normal
- Urinalysis: Presence of leukocytes and bacteria
- Urine culture: Positive for Escherichia coli
These findings confirmed recurrent urinary tract infection with preserved overall renal function due to a functioning contralateral kidney.
Diagnosis
A definitive diagnosis of unilateral renal atresia (left-sided ureteral atresia) with secondary hydronephrosis and renal dysplasia was established based on imaging and functional studies.
The absence of ureteral continuity, severe hydronephrosis, and poor renal function confirmed the diagnosis.
Management and Outcome
Management Strategy
The treatment plan focused on:
- Preventing recurrent infections
- Preserving contralateral kidney function
- Addressing the non-functioning kidney
- Long-term monitoring of renal health
Medical Management
The child was started on appropriate intravenous antibiotics based on culture sensitivity, followed by oral prophylactic antibiotics to reduce recurrence.
Hydration and nutritional support were maintained.
Surgical Management
Given the negligible function of the affected kidney and risk of recurrent infection, a left-sided nephrectomy was performed.
The procedure was uneventful, and postoperative recovery was smooth.
Post-Treatment Course
The child showed significant clinical improvement following surgery, with resolution of fever and abdominal symptoms. No further episodes of urinary tract infection were reported.
Follow-Up
At 1 Month
The patient remained asymptomatic. Surgical site healing was satisfactory. Renal function tests were within normal limits.
At 3 Months
Ultrasound showed a normal right kidney with compensatory hypertrophy. No abnormalities were noted.
At 6 Months
The child continued to thrive well with normal growth parameters and stable renal function.
Discussion
Pathophysiology
Renal atresia results from developmental failure of the ureteric bud or interruption in its canalization during embryogenesis. This leads to obstruction of urine flow, resulting in progressive dilation of the renal pelvis and calyces (hydronephrosis).
Prolonged obstruction causes increased intrarenal pressure, leading to ischemia, tubular atrophy, and eventual renal dysplasia.
Etiology and Risk Factors
The exact cause of renal atresia remains unclear, but several contributing factors include:
- Genetic mutations affecting urinary tract development
- Abnormal interaction between ureteric bud and metanephric blastema
- Intrauterine vascular insults
- Associated congenital anomalies
Epidemiology
Renal atresia is a rare condition, often identified in infancy or early childhood. It is more commonly unilateral, with bilateral cases being incompatible with life due to severe renal failure.
Clinical Manifestations
Symptoms depend on the severity and laterality:
- Recurrent urinary tract infections
- Abdominal or flank mass
- Pain or discomfort
- Failure to thrive in severe cases
- Asymptomatic (detected incidentally)
In this case, recurrent infections and abdominal findings led to diagnosis.
Diagnostic Considerations
Early diagnosis relies on imaging modalities:
- Ultrasound: Initial screening tool
- MR Urography: Provides detailed anatomical visualization
- Nuclear Scan: Assesses renal function
- VCUG: Rules out reflux
These investigations help differentiate renal atresia from other obstructive uropathies.
Treatment Considerations
Conservative Management
In cases where renal function is preserved, monitoring and infection control may be sufficient.
Surgical Intervention
Indicated when:
- Kidney function is severely compromised
- Recurrent infections occur
- Risk of complications is high
Procedures include:
- Pyeloplasty (if partial obstruction)
- Nephrectomy (non-functioning kidney)
Emerging Approaches
Advances in pediatric urology include:
- Minimally invasive laparoscopic surgeries
- Improved prenatal diagnosis
- Genetic screening for congenital anomalies
- Tissue engineering for renal regeneration
Complications
Untreated renal atresia can lead to:
- Recurrent infections
- Hypertension
- Chronic kidney disease
- Renal failure (in bilateral cases)
Prognosis
The prognosis is excellent in unilateral cases with a healthy contralateral kidney. Early intervention prevents long-term complications and ensures normal growth and development.
Conclusion
Renal atresia is a rare but significant congenital anomaly that requires prompt recognition and appropriate management. This case underscores the importance of early diagnosis through imaging and timely surgical intervention in preventing recurrent infections and preserving overall renal function.
Regular follow-up and monitoring of the functioning kidney are essential to ensure long-term health and prevent complications. Advances in diagnostic and surgical techniques continue to improve outcomes in pediatric patients with congenital renal anomalies.
References
- Woolf AS, et al. Congenital abnormalities of the kidney and urinary tract. https://pubmed.ncbi.nlm.nih.gov/21496972/
- Chevalier RL. Pathogenesis of renal injury in obstructive uropathy. https://pubmed.ncbi.nlm.nih.gov/15213341/
- Nguyen HT, et al. Evaluation and management of hydronephrosis. https://pubmed.ncbi.nlm.nih.gov/20303509/
- National Kidney Foundation. Pediatric kidney disorders. https://www.kidney.org/
- Elder JS. Congenital anomalies of the urinary tract. https://pubmed.ncbi.nlm.nih.gov/12831669/
- Rabelo EA, et al. Role of MR urography in pediatric urology. https://pubmed.ncbi.nlm.nih.gov/19457876/
- Koff SA. Neonatal management of urinary tract obstruction. https://pubmed.ncbi.nlm.nih.gov/15283368/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge