Cervical Cancer: Diagnostic Pathways, Multimodal Treatment, and Clinical Outcomes - A Case Report
OthersPage Navigation
Abstract
Cervical cancer remains a major public health concern worldwide, particularly in low- and middle-income countries, despite being largely preventable through screening and human papillomavirus (HPV) vaccination. The disease often presents insidiously, with early-stage cancer remaining asymptomatic and advanced disease manifesting with gynecological, urinary, or systemic symptoms. Timely diagnosis and stage-appropriate management are critical determinants of survival and quality of life. We report a case of locally advanced cervical cancer in a middle-aged woman who presented with abnormal uterine bleeding and pelvic discomfort. Comprehensive clinical evaluation, histopathological confirmation, and radiological staging established the diagnosis of squamous cell carcinoma of the cervix. The patient was managed with definitive concurrent chemoradiation, resulting in favorable clinical and radiological response. This case underscores the importance of early recognition, standardized staging, and multidisciplinary management in optimizing outcomes for cervical cancer patients.
Introduction
Cervical cancer is the fourth most common malignancy among women globally and a leading cause of cancer-related mortality in developing regions [1]. Persistent infection with high-risk human papillomavirus (HPV), particularly HPV types 16 and 18, is the principal etiological factor, accounting for over 95% of cases [2]. Despite the availability of effective screening methods such as Papanicolaou (Pap) smear testing and HPV DNA testing, many patients continue to present with advanced disease due to inadequate screening coverage and limited access to healthcare services.
The natural history of cervical cancer typically involves progression from cervical intraepithelial neoplasia to invasive carcinoma over several years, providing a substantial window for early detection and intervention. However, once invasive cancer develops, management becomes complex and is guided by disease stage, histology, and patient-related factors. Standard treatment modalities include surgery, radiotherapy, chemotherapy, or combinations thereof [3].
This case report describes the clinical presentation, diagnostic evaluation, staging, and management of a patient with locally advanced cervical cancer, highlighting diagnostic challenges and principles of contemporary treatment.
Case Report
Patient History
A 48-year-old woman presented to the gynecology outpatient clinic with complaints of irregular vaginal bleeding and postcoital spotting for the past four months. She also reported dull lower abdominal pain and occasional foul-smelling vaginal discharge. There was no history of significant weight loss, loss of appetite, or bowel and bladder disturbances.
Her obstetric history included three full-term vaginal deliveries. She had not undergone regular gynecological screening and had never received HPV vaccination. There was no history of oral contraceptive use, smoking, or sexually transmitted infections. Her medical history was otherwise unremarkable, with no known chronic illnesses or prior surgeries.
Clinical Examination
On general examination, the patient was hemodynamically stable, with mild pallor noted. Abdominal examination revealed mild suprapubic tenderness without palpable masses. Pelvic examination demonstrated an irregular, friable cervical growth that bled on contact. The lesion appeared to involve the cervix circumferentially, with limited mobility of the cervix on bimanual examination, raising concern for parametrial involvement.

No clinically enlarged inguinal or supraclavicular lymph nodes were detected. Rectovaginal examination suggested mild induration of the left parametrium, while the rectal mucosa appeared uninvolved.
Investigations
Laboratory Evaluation
Baseline laboratory investigations revealed mild anemia, with a hemoglobin level of 9.8 g/dL. Renal and liver function tests were within normal limits. Serological testing for HIV was negative.
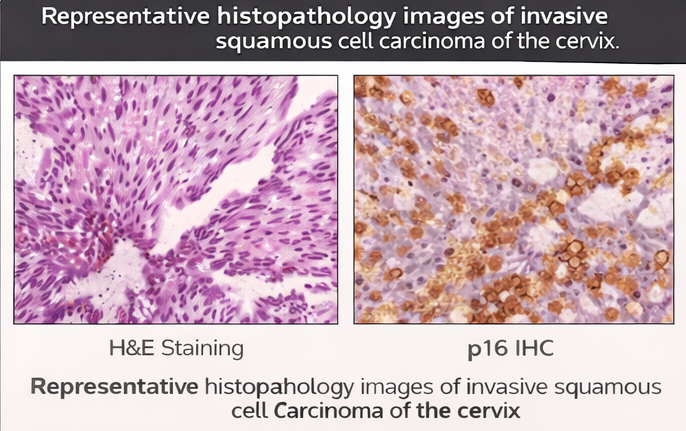
Histopathological Assessment
A punch biopsy from the cervical lesion was performed. Histopathological examination demonstrated invasive squamous cell carcinoma, moderately differentiated, with evidence of stromal invasion. Immunohistochemical staining supported the diagnosis, with tumor cells showing p16 positivity, consistent with HPV-associated malignancy.
Radiological Staging
Pelvic magnetic resonance imaging (MRI) revealed a cervical mass measuring approximately 4.5 cm in greatest dimension, extending into the left parametrium without involvement of the pelvic sidewall. The uterus and upper vagina were partially involved, while the bladder and rectum appeared free of tumor infiltration.
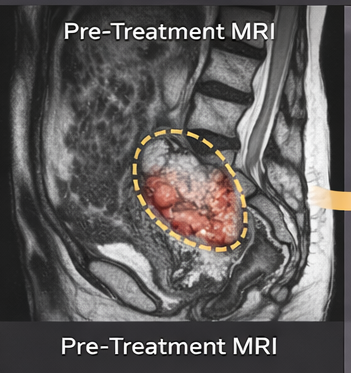
Contrast-enhanced computed tomography (CT) of the abdomen and pelvis showed no evidence of distant metastases or para-aortic lymphadenopathy. Chest imaging was unremarkable. Based on clinical and radiological findings, the disease was staged as FIGO stage IIB cervical cancer.
Diagnosis
Based on clinical findings, histopathological confirmation, and radiological staging, a diagnosis of locally advanced cervical squamous cell carcinoma (FIGO stage IIB) was established.
Management and Outcome
The patient was discussed at a multidisciplinary tumor board comprising gynecologic oncologists, radiation oncologists, medical oncologists, radiologists, and pathologists. In accordance with international guidelines, definitive concurrent chemoradiation was recommended as the standard of care for stage IIB cervical cancer [4].
Treatment
The patient underwent external beam radiotherapy (EBRT) to the pelvis, receiving a total dose of 50 Gy in 25 fractions over five weeks. This was administered concurrently with weekly cisplatin chemotherapy at a dose of 40 mg/m². Following EBRT, she received high-dose-rate intracavitary brachytherapy, delivering an equivalent dose to the cervix and parametrium.
Supportive care measures included correction of anemia with iron supplementation, nutritional counseling, and proactive management of treatment-related side effects. The patient tolerated therapy reasonably well, with manageable gastrointestinal symptoms and mild hematological toxicity.
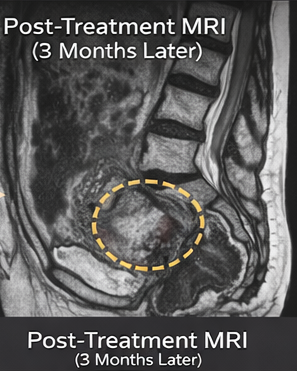
Follow-Up
At three months post-treatment, clinical examination showed complete resolution of the cervical lesion. MRI of the pelvis demonstrated significant tumor regression with no residual disease. At six-month follow-up, the patient remained asymptomatic, with no evidence of local recurrence or distant metastasis. Menopausal symptoms related to pelvic irradiation were managed conservatively.
Discussion
Cervical cancer remains a preventable yet prevalent malignancy, particularly in populations with limited access to screening and vaccination programs. This case illustrates a typical presentation of locally advanced disease in a woman who had not undergone regular cervical screening, emphasizing the consequences of delayed detection.
Abnormal vaginal bleeding remains the most common presenting symptom of cervical cancer, especially in advanced stages. Clinical examination and biopsy are essential for diagnosis, while MRI plays a critical role in local staging due to its superior soft tissue resolution [5].
Concurrent chemoradiation has become the cornerstone of treatment for locally advanced cervical cancer, with multiple randomized trials demonstrating improved survival compared to radiotherapy alone [6]. Cisplatin-based chemotherapy enhances radiosensitivity and improves local control and overall survival.
Despite effective treatment, long-term surveillance is essential due to the risk of recurrence and late radiation-related complications. Survivorship care should also address psychosocial, sexual, and quality-of-life concerns, which are often underrecognized in cervical cancer patients.
Conclusion
Cervical cancer continues to pose a significant clinical challenge, particularly in women who lack access to preventive screening and early diagnosis. This case highlights the importance of prompt evaluation of abnormal gynecological symptoms, standardized staging, and evidence-based multimodal therapy.
Early detection through screening and widespread HPV vaccination remains the most effective strategy to reduce cervical cancer incidence and mortality. For patients with established disease, a coordinated multidisciplinary approach is essential to achieve optimal oncological and functional outcomes.
References
- World Health Organization. Cervical cancer. WHO Fact Sheet. 2023.
- Walboomers JM, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189(1):12–19.
- Bhatla N, et al. Revised FIGO staging for carcinoma of the cervix uteri. Int J Gynecol Obstet. 2019;145(1):129–135.
- National Comprehensive Cancer Network (NCCN). Cervical Cancer Guidelines. Version 2024.
- Sala E, et al. MRI of cervical cancer: staging and assessment of response to treatment. AJR Am J Roentgenol. 2007;189(6):1553–1562.
- Green JA, et al. Concomitant chemotherapy and radiation therapy for cancer of the uterine cervix. Cochrane Database Syst Rev. 2005;(3):CD002225.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Year in Review: Chronic Lymphocytic Leukemia
2.
According to a study, white Americans are overdiagnosing melanoma at an alarming rate.
3.
Approval in Endometrial Cancer Expanded; Masks at Cancer Centers; NPR Reporter Dies
4.
The First Gene Therapy Provides a Durable Response for Non-Muscle-Invasive Bladder Cancer.
5.
Canine Cancer Vaccine: A Potential Resurrection? U.S. KK. Snubs Enertu.
1.
What Is Carboxyhemoglobin And How Can It Affect Your Health?
2.
Lu-177 Vipivotide in Prostate Cancer: A Breakthrough in Radioligand Therapy
3.
Unraveling the Mysteries of Coagulopathy: A Comprehensive Definition
4.
Machine Learning in Genomic Analysis for Early Lung Cancer Detection: Key Advances and Insights
5.
A New Perspective on Spherocytosis: Uncovering Innovative Treatments
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Updates on the First Line Management of ALK+ NSCLC
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part II

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge