Cutaneous Larva Migrans (Ancylostoma braziliense): Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Cutaneous larva migrans (CLM), commonly caused by Ancylostoma braziliense, is a parasitic skin infection characterized by serpiginous, pruritic skin lesions resulting from the migration of hookworm larvae within the epidermis. It is frequently associated with exposure to contaminated soil or sand, particularly in tropical and subtropical regions. Although the condition is self-limiting, it can cause significant discomfort and secondary complications due to intense itching. Diagnosis is primarily clinical, and treatment with antihelminthic agents leads to rapid resolution. This case report describes an adult patient with typical CLM, highlighting clinical features, diagnostic approach, management, and favorable outcome following pharmacological therapy.
Introduction
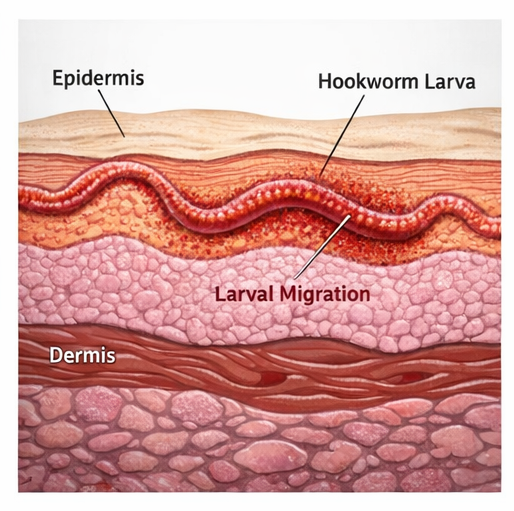
Cutaneous larva migrans is a zoonotic parasitic infection caused predominantly by the larvae of animal hookworms, most commonly Ancylostoma braziliense. Humans are incidental hosts, and the larvae are unable to penetrate beyond the epidermis, resulting in characteristic cutaneous manifestations.
The infection typically occurs through direct contact with contaminated soil or sand, especially in areas frequented by dogs and cats. Risk factors include walking barefoot, occupational exposure, and recreational activities such as beach visits.
Pathophysiologically, the larvae penetrate intact skin and migrate within the superficial layers, producing a serpiginous track due to their movement. The host immune response contributes to inflammation and intense pruritus.

Clinically, CLM is usually benign but highly symptomatic. Without treatment, the larvae eventually die within weeks; however, early intervention is recommended to relieve symptoms and prevent complications such as secondary bacterial infection.
Case Report
Patient History
A 35-year-old male presented to the dermatology outpatient department with complaints of an intensely itchy, progressively spreading skin lesion over the right foot for 10 days.
The patient reported that the lesion began as a small red papule, which gradually extended into a winding, linear track. The itching was severe, particularly at night, interfering with sleep.

He had recently returned from a coastal area where he frequently walked barefoot on the beach. There was no history of trauma, insect bites, or prior similar episodes.

There were no systemic symptoms such as fever, malaise, or gastrointestinal complaints. The patient had no significant past medical history and was not on any regular medications.
Clinical Examination
On examination, the patient was afebrile and hemodynamically stable.
Local examination of the right foot revealed:
- A raised, erythematous, serpiginous track measuring approximately 5 cm in length
- The lesion had a slightly elevated border with a linear, winding pattern
- Evidence of excoriation due to scratching
- No signs of secondary infection such as pus, warmth, or swelling
The lesion appeared to have advanced compared to the patient’s initial description, suggesting active larval migration.
Systemic examination was unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
- Cutaneous larva migrans
- Scabies (atypical presentation)
- Contact dermatitis
- Tinea corporis
- Larva currens (Strongyloides infection)
The characteristic serpiginous track, history of beach exposure, and intense pruritus strongly suggested CLM.
Investigations
Laboratory Findings
Routine laboratory investigations were within normal limits:
- Complete blood count: Normal, with no significant eosinophilia
- No evidence of systemic infection
Imaging and Diagnostic Tests
No imaging studies were required, as diagnosis was clinical. Skin biopsy was not performed due to the transient nature of the larvae and typical presentation.
Diagnosis
Based on clinical features and exposure history, the diagnosis was established as:
Cutaneous Larva Migrans caused by Ancylostoma braziliense
Management and Outcome
Initial Management
The patient was started on pharmacological therapy:
- Oral albendazole 400 mg once daily for 3 days
- Oral antihistamines for symptomatic relief of itching
Topical soothing agents were also prescribed to reduce local irritation.
The patient was advised:
- To avoid scratching to prevent secondary infection
- To maintain proper hygiene
- About the benign nature of the condition
Follow-Up Management
The patient was reviewed after one week:
- Significant reduction in itching
- Arrest of lesion progression
- Beginning of lesion resolution
At two-week follow-up:
- Complete resolution of the serpiginous track
- No residual pigmentation or scarring
- No recurrence of symptoms
Outcome
The patient showed excellent response to treatment:
- Rapid symptomatic relief within days
- Complete clinical resolution within two weeks
- No complications or recurrence observed

Discussion
Cutaneous larva migrans is the most common dermatological manifestation of hookworm infection in humans. It is primarily caused by Ancylostoma braziliense, a parasite commonly found in dogs and cats.
Transmission occurs when infective larvae in contaminated soil penetrate the skin. Since humans are not the natural host, the larvae are unable to complete their lifecycle and remain confined to the epidermis.
The hallmark feature is a creeping eruption, characterized by a serpiginous, erythematous track that advances daily. Intense pruritus is a defining symptom and can significantly affect quality of life.
Diagnosis is clinical, based on:
- Characteristic lesion morphology
- History of exposure
- Absence of systemic involvement
Laboratory and imaging studies are generally not required. Biopsy is rarely helpful, as the larva is often not captured.
Management focuses on:
- Eradication of the larvae
- Symptomatic relief
First-line treatments include:
- Albendazole
- Ivermectin
These agents are highly effective and lead to rapid resolution. Antihistamines help control pruritus, while topical treatments provide additional comfort.
Complications are uncommon but may include:
- Secondary bacterial infection due to scratching
- Persistent itching
- Rarely, systemic hypersensitivity reactions
Prevention is essential and includes:
- Avoiding barefoot walking in endemic areas
- Maintaining hygiene in public spaces
- Proper deworming of pets
The prognosis is excellent, especially with early treatment. Even untreated cases eventually resolve, but therapy significantly reduces morbidity.
This case highlights the importance of recognizing classical clinical features and initiating prompt treatment to ensure rapid recovery and patient comfort.
Conclusion
Cutaneous larva migrans caused by Ancylostoma braziliense is a common parasitic skin infection in adults with exposure to contaminated environments. It presents with characteristic serpiginous, pruritic lesions and is primarily diagnosed clinically. Early treatment with antihelminthic agents leads to rapid symptom resolution and prevents complications. This case emphasizes the importance of clinical awareness, appropriate management, and preventive measures in achieving favorable outcomes.
References
- Caumes E. Treatment of cutaneous larva migrans. https://pubmed.ncbi.nlm.nih.gov/10485535/
- Heukelbach J, Feldmeier H. Epidemiological and clinical characteristics of hookworm-related cutaneous larva migrans. https://pubmed.ncbi.nlm.nih.gov/15364248/
- Hochedez P, Caumes E. Hookworm-related cutaneous larva migrans. https://pubmed.ncbi.nlm.nih.gov/17205498/
- Blackwell V, Vega-Lopez F. Cutaneous larva migrans: clinical features and management. https://pubmed.ncbi.nlm.nih.gov/16634846/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge