Intraocular Foreign Body: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Intraocular foreign body (IOFB) is a vision-threatening ophthalmic emergency characterized by the retention of a foreign object within the globe following penetrating trauma. It is a significant cause of ocular morbidity, particularly among young working-age males engaged in high-risk occupations. The clinical spectrum ranges from mild visual disturbance to severe vision loss depending on the size, location, and composition of the foreign body.
We report the case of a 32-year-old male who presented with acute visual impairment following occupational trauma. Imaging revealed a metallic intraocular foreign body lodged in the posterior segment. The patient underwent prompt surgical intervention with favorable anatomical and functional recovery.
This case highlights the importance of early diagnosis, appropriate imaging, and timely surgical management to prevent complications such as endophthalmitis, retinal detachment, and toxic ocular reactions.
Introduction
Intraocular foreign body (IOFB) refers to the presence of an exogenous material within the eye following a penetrating injury. Such injuries are commonly associated with high-velocity mechanisms, including hammering, drilling, or industrial accidents.
The nature of the retained object significantly influences the clinical course. Metallic foreign bodies may cause toxic effects such as siderosis bulbi (iron deposition) or chalcosis (copper deposition), whereas organic materials increase the risk of severe intraocular infection, including endophthalmitis.
IOFB injuries are more prevalent in developing regions where occupational safety measures, such as protective eyewear, are inconsistently used. Early recognition and management are critical, as delays can result in irreversible vision loss.
Case Report
Patient History
A 32-year-old male presented to the emergency department with the following complaints:
• Sudden decrease in vision in the right eye following a metal grinding injury
• Ocular pain and redness
• Foreign body sensation
• Mild photophobia
The patient reported that the injury occurred at his workplace while grinding metal without protective goggles. There was no history of prior ocular disease, systemic illness, or similar episodes.
Clinical Examination
General Examination
• Patient conscious and hemodynamically stable
• No systemic abnormalities
Ocular Examination
• Visual acuity: Counting fingers close to face (right eye)
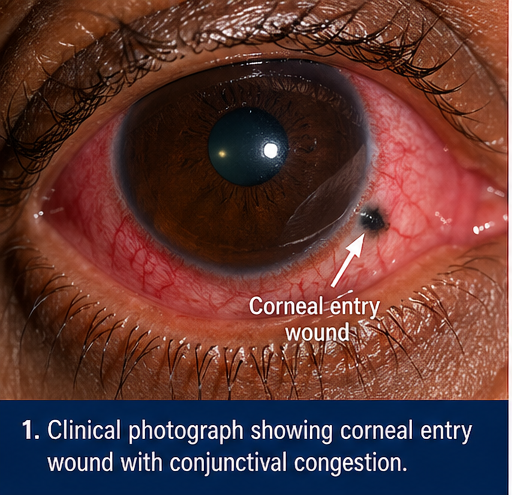
• Conjunctival congestion and ciliary injection
• Small, self-sealed corneal entry wound
• Anterior chamber: Mild inflammatory reaction
• Pupil: Sluggishly reactive
Posterior Segment
• Fundus examination not clearly visualized due to media opacity, likely secondary to vitreous hemorrhage
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following were considered:
• Intraocular foreign body
• Penetrating globe injury without retained foreign body
• Traumatic cataract
• Vitreous hemorrhage
The history of high-velocity trauma strongly indicated the likelihood of a retained intraocular foreign body.
Investigations
Laboratory Tests
• Routine blood investigations: Within normal limits
• No signs of systemic infection
Imaging
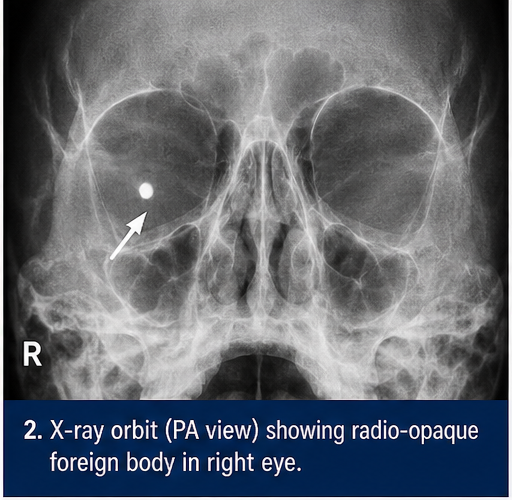
X-ray Orbit
• Radio-opaque foreign body identified
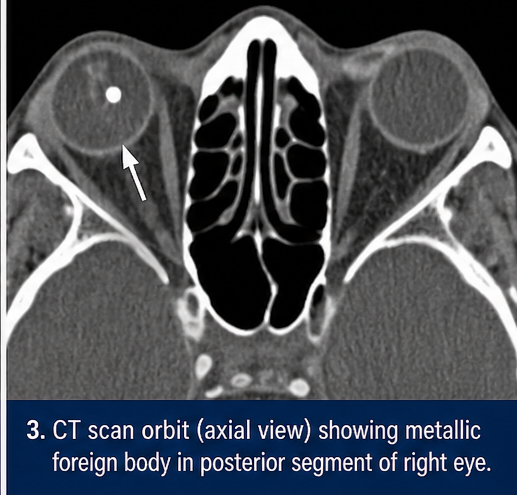
CT Scan Orbit (Gold Standard)
• Hyperdense metallic foreign body in the posterior segment
• No orbital fractures
• Globe integrity maintained
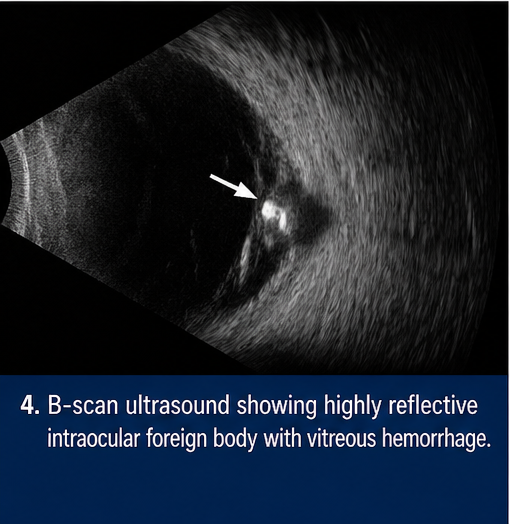
Ultrasound B-Scan
• Highly reflective intraocular echo suggestive of foreign body
• Associated vitreous hemorrhage
MRI was avoided due to the risk of movement of the metallic foreign body.
Diagnosis
A definitive diagnosis of posterior segment intraocular foreign body was established based on clinical findings and radiological imaging. The identification of a metallic object within the vitreous cavity, along with a consistent history of penetrating trauma, confirmed the diagnosis and ruled out alternative causes.
Management and Outcome
Management Strategy
The treatment plan was individualized based on:
• Location and size of the foreign body
• Material composition
• Presence of complications such as hemorrhage or infection
Surgical Management
Primary Wound Repair
• Closure of corneal entry site to restore globe integrity
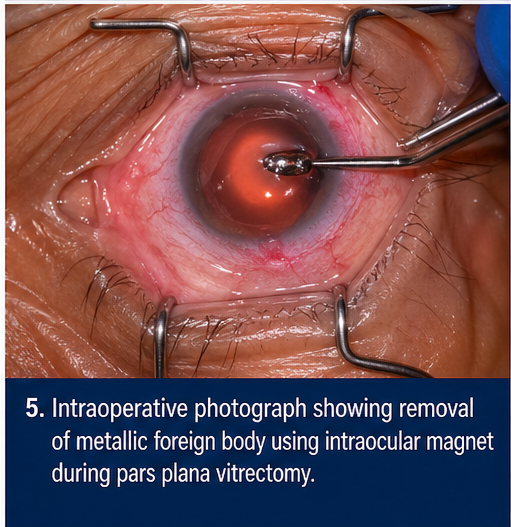
Pars Plana Vitrectomy (PPV)
• Removal of vitreous hemorrhage
• Extraction of foreign body using intraocular magnet
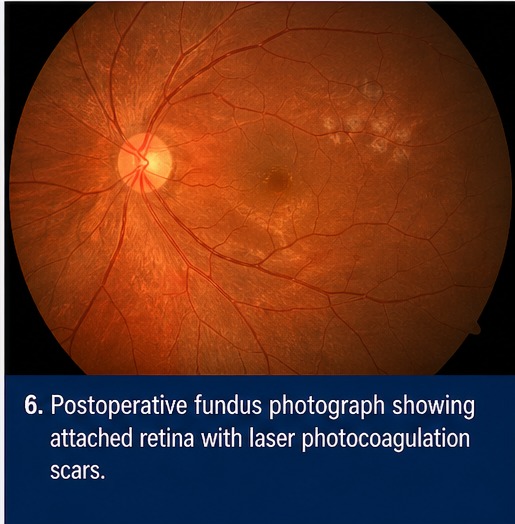
Adjunctive Procedures
• Endolaser photocoagulation to stabilize retina
• Intravitreal antibiotics to prevent endophthalmitis
Medical Management
• Systemic broad-spectrum antibiotics
• Topical antibiotics and corticosteroids
• Cycloplegic agents to reduce ciliary spasm
Clinical Course
During hospitalization:
• Ocular inflammation reduced progressively
• No signs of infection or worsening pathology
• Visual acuity began improving gradually
Follow-Up
At 2 Weeks
• Reduced inflammation
• Improved visual acuity
At 1 Month
• Retina attached
• No residual foreign body
At 3 Months
• Stable anatomical outcome
• Functional visual recovery achieved
• No complications such as retinal detachment or siderosis
The patient resumed daily activities with strict advice on occupational eye safety.
Discussion
Pathophysiology
Intraocular foreign bodies enter the globe through penetrating trauma and may damage multiple ocular structures. The impact can cause:
• Mechanical disruption of tissues
• Hemorrhage within ocular compartments
• Secondary inflammatory response
The composition of the foreign body determines toxicity:
• Iron → Siderosis bulbi
• Copper → Chalcosis
• Organic matter → Severe infection risk
Epidemiology
• Predominantly affects males aged 20–40 years
• Common in industrial and construction workers
• Strong association with lack of protective eyewear
Clinical Manifestations
Anterior Segment Findings
• Corneal entry wound
• Hyphema
• Anterior chamber reaction
Posterior Segment Findings
• Vitreous hemorrhage
• Retinal tears or detachment
• Intraocular foreign body on imaging
Diagnostic Considerations
Accurate diagnosis relies on:
• Detailed trauma history
• Comprehensive ocular examination
• Imaging modalities
CT scan is the gold standard for detecting and localizing IOFBs, especially metallic ones. Ultrasound is useful when fundus visualization is limited. MRI is contraindicated in suspected metallic IOFBs due to the risk of movement and further damage.
Treatment Considerations
Primary Objectives
• Safe removal of foreign body
• Prevention of infection
• Preservation of visual function
Indications for Surgical Removal
• Posterior segment foreign bodies
• Toxic or reactive materials
• Associated complications
Complications
• Endophthalmitis
• Retinal detachment
• Cataract formation
• Siderosis bulbi
• Permanent vision loss
Prognosis
The visual outcome depends on several factors:
• Initial visual acuity
• Time interval between injury and intervention
• Location of foreign body
• Presence of complications
Early diagnosis and prompt surgical management significantly improve outcomes.
Conclusion
Intraocular foreign body is a critical ophthalmic emergency that requires a high index of suspicion, particularly in occupational injuries involving high-velocity mechanisms.
This case demonstrates that timely imaging, early surgical intervention, and appropriate postoperative care can result in excellent anatomical and functional recovery. Preventive strategies, including the consistent use of protective eyewear, remain essential in reducing the incidence of such injuries.
Early diagnosis, individualized treatment, and regular follow-up are key to preventing complications and ensuring optimal visual outcomes.
References
-
Kuhn F, Morris R, Witherspoon CD. Intraocular foreign bodies. Ophthalmology Clinics. https://pubmed.ncbi.nlm.nih.gov/17011951/
-
Essex RW, Yi Q, Charles PG, Allen PJ. Post-traumatic endophthalmitis. Ophthalmology. https://pubmed.ncbi.nlm.nih.gov/15177960/
-
Loporchio D, Mukkamala L, Gorukanti K, et al. Intraocular foreign bodies: A review. Eye (Lond). https://pubmed.ncbi.nlm.nih.gov/26688138/
-
American Academy of Ophthalmology. Open Globe Injury Guidelines. https://www.aao.org
-
World Health Organization. Prevention of Blindness due to Eye Injuries. https://www.who.int
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge