Aneurysm: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
An aneurysm is an abnormal localized dilatation of a blood vessel caused by weakening of the vessel wall. Aneurysms most commonly involve the aorta and cerebral arteries and may remain asymptomatic until rupture or compression of adjacent structures occurs. Ruptured aneurysms are associated with high morbidity and mortality and therefore require prompt diagnosis and management. Risk factors include hypertension, smoking, atherosclerosis, genetic disorders, ageing, and connective tissue abnormalities.
We present the case of a 58-year-old male who presented with sudden severe headache, vomiting, and transient loss of consciousness. Neurological evaluation and imaging studies revealed a ruptured cerebral aneurysm causing subarachnoid hemorrhage. The patient underwent emergency endovascular coiling followed by intensive supportive care and rehabilitation, resulting in gradual neurological recovery.
This case highlights the importance of early recognition, rapid neuroimaging, and timely intervention in reducing complications and improving outcomes in patients with aneurysmal rupture.
Introduction
An aneurysm refers to a pathological ballooning or dilatation of an artery resulting from weakening of the vascular wall. Depending on the location, aneurysms may involve:
-
Cerebral arteries
-
Abdominal aorta
-
Thoracic aorta
-
Peripheral arteries
Cerebral aneurysms are among the most clinically significant types because rupture may lead to subarachnoid hemorrhage, stroke, permanent neurological deficits, or death.
Aneurysms are classified into:
-
Saccular aneurysm
-
Fusiform aneurysm
-
Dissecting aneurysm
-
Pseudoaneurysm
The pathogenesis involves progressive degeneration of the vessel wall caused by:
-
Hypertension
-
Atherosclerosis
-
Smoking
-
Connective tissue disorders
-
Genetic predisposition
-
Inflammatory vascular injury
Small aneurysms may remain asymptomatic for years and are often detected incidentally during imaging studies. However, rupture can result in catastrophic bleeding and requires immediate medical attention.
The prevalence of intracranial aneurysms in the general population is estimated to be approximately 2–5%. Risk increases with advancing age, smoking, uncontrolled hypertension, and family history.
Early diagnosis and intervention play a crucial role in reducing morbidity and mortality associated with aneurysmal disease.
Case Report
Patient History
A 58-year-old male presented to the emergency department with:
-
Sudden onset severe headache described as “worst headache of life”
-
Vomiting
-
Brief loss of consciousness
-
Neck stiffness
-
Dizziness and photophobia
The symptoms began abruptly while the patient was at home.
Medical history revealed:
-
Hypertension for 10 years
-
Chronic smoking history
-
Dyslipidemia
-
Poor compliance with antihypertensive medications
There was no previous history of stroke, seizures, or head trauma.
Family history revealed hypertension in both parents but no known cerebrovascular disease.
Clinical Examination
General Examination
-
Patient drowsy but arousable
-
Blood pressure: 180/100 mmHg
-
Pulse rate: 96/min
-
Respiratory rate: 20/min
-
Afebrile
Neurological Examination
-
Neck rigidity present
-
Positive Kernig’s sign
-
Mild confusion
-
No focal motor weakness
-
Pupils equal and reactive
Cardiovascular and respiratory examinations were otherwise unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on the presentation, the following conditions were considered:
-
Subarachnoid hemorrhage
-
Ruptured cerebral aneurysm
-
Hypertensive intracranial bleed
-
Meningitis
-
Ischemic stroke
-
Cerebral venous thrombosis
The sudden thunderclap headache strongly suggested aneurysmal subarachnoid hemorrhage.
Investigations
Routine Laboratory Tests
-
Complete blood count: Normal
-
Blood glucose: Mildly elevated
-
Renal function tests: Normal
-
Coagulation profile: Normal
Neuroimaging
CT Scan Brain
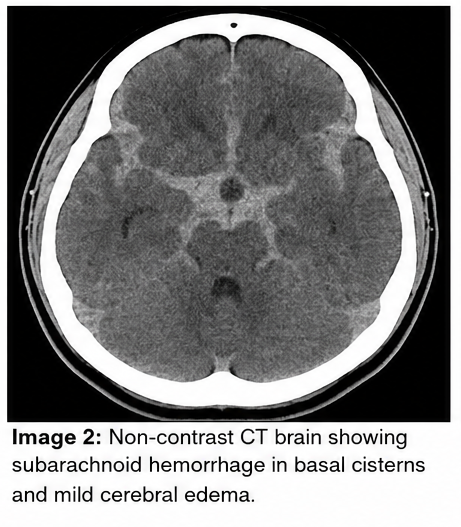
Non-contrast CT brain revealed:
-
Subarachnoid hemorrhage in basal cisterns
-
Mild cerebral edema
-
No significant midline shift
CT Angiography
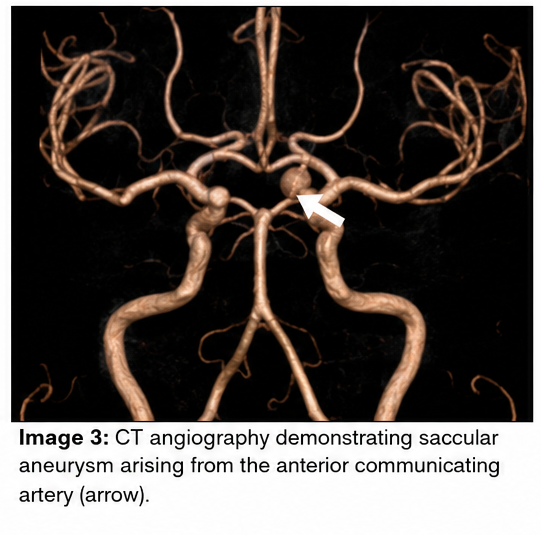
CT angiography demonstrated:
-
Saccular aneurysm arising from the anterior communicating artery
-
Aneurysm size approximately 6 mm
-
No additional vascular malformations
Lumbar Puncture
Not performed due to positive CT findings.
Diagnosis
Based on clinical presentation and imaging findings, the diagnosis of: Ruptured Intracranial Saccular Aneurysm with Subarachnoid Hemorrhage was established.
Management and Outcome
Initial Stabilization
The patient was admitted to the intensive care unit and managed with:
-
Blood pressure control
-
Intravenous fluids
-
Pain management
-
Nimodipine therapy
-
Neurological monitoring
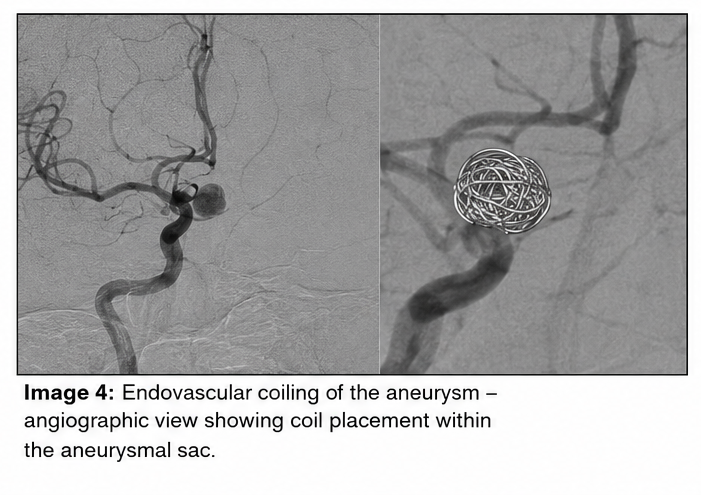
Definitive Treatment
The patient underwent emergency endovascular coiling of the aneurysm to prevent rebleeding.
The procedure was completed successfully without intraoperative complications.
Post-Procedural Care
Postoperative management included:
-
Monitoring for vasospasm
-
Electrolyte correction
-
Seizure prophylaxis
-
Physiotherapy and rehabilitation
Clinical Course
At 48 Hours
-
Headache significantly reduced
-
Consciousness improved
-
No new neurological deficits
At 1 Week
-
Neck rigidity resolved
-
Stable neurological status
-
Repeat imaging showed no rebleeding
At 1 Month Follow-Up
-
Independent daily activities resumed
-
Mild fatigue persisted
-
No focal neurological deficits
-
Blood pressure well controlled
Discussion
Pathophysiology
Aneurysms develop due to structural weakness in the arterial wall leading to progressive vessel dilatation. Degeneration of elastic tissue and smooth muscle contributes to aneurysm formation.
Important mechanisms include:
-
Hemodynamic stress
-
Endothelial dysfunction
-
Chronic hypertension
-
Atherosclerotic damage
-
Inflammatory vascular injury
Cerebral aneurysms most commonly occur at arterial bifurcations within the Circle of Willis where blood flow turbulence is greatest.
Epidemiology
Key epidemiological features include:
-
Intracranial aneurysms affect approximately 2–5% of the population
-
More common in adults above 40 years
-
Higher prevalence in females
-
Smoking and hypertension are major risk factors
-
Rupture incidence increases with aneurysm size
Subarachnoid hemorrhage secondary to aneurysm rupture carries substantial mortality and long-term disability.
Clinical Manifestations
Unruptured Aneurysm
Small aneurysms may remain asymptomatic. Symptomatic cases may present with:
-
Headache
-
Visual disturbances
-
Cranial nerve palsy
-
Facial pain
-
Dizziness
Ruptured Aneurysm
Typical manifestations include:
-
Sudden severe headache
-
Vomiting
-
Neck stiffness
-
Altered consciousness
-
Photophobia
-
Seizures
The classic “thunderclap headache” is highly suggestive of subarachnoid hemorrhage.
Diagnostic Considerations
Diagnosis requires prompt imaging evaluation. Important diagnostic tools include:
-
Non-contrast CT brain
-
CT angiography
-
Magnetic resonance angiography
-
Digital subtraction angiography
-
Lumbar puncture when CT is inconclusive
CT angiography provides rapid visualization of aneurysm anatomy and guides treatment planning.
Treatment Modalities
Medical Management
Initial supportive care includes:
-
Blood pressure control
-
Prevention of vasospasm
-
Pain management
-
Seizure prevention
-
Intensive monitoring
Surgical Management
Definitive treatment options include:
-
Surgical clipping
-
Endovascular coiling
-
Flow-diverting stents
Endovascular therapy is increasingly preferred due to reduced invasiveness and shorter recovery time.
Complications
Potential complications include:
-
Rebleeding
-
Cerebral vasospasm
-
Hydrocephalus
-
Stroke
-
Seizures
-
Cognitive impairment
-
Death
Delayed cerebral ischemia remains a major cause of neurological deterioration following aneurysmal rupture.
Prognosis
Prognosis depends on:
-
Size and location of aneurysm
-
Time to intervention
-
Severity of hemorrhage
-
Patient age
-
Neurological status at presentation
Early diagnosis and timely intervention significantly improve survival and neurological recovery.
In this case, rapid neuroimaging and emergency endovascular treatment resulted in favorable clinical outcome and prevention of recurrent hemorrhage.
Conclusion
Aneurysms are potentially life-threatening vascular abnormalities that require early identification and prompt management. Ruptured cerebral aneurysms can rapidly lead to severe neurological complications and high mortality if untreated.
This case highlights the importance of recognizing warning symptoms such as sudden severe headache and utilizing rapid neuroimaging for accurate diagnosis. Early intervention with endovascular or surgical techniques remains essential for improving patient outcomes and reducing long-term neurological disability.
Comprehensive management involving intensive monitoring, blood pressure control, prevention of vasospasm, and rehabilitation plays a critical role in successful recovery.
References
-
Connolly ES Jr, Rabinstein AA, Carhuapoma JR, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage. https://pubmed.ncbi.nlm.nih.gov/22556195/
-
Brown RD Jr, Broderick JP. Unruptured intracranial aneurysms: epidemiology, natural history, management options, and familial screening. https://pubmed.ncbi.nlm.nih.gov/17261669/
-
Thompson BG, Brown RD Jr, Amin-Hanjani S, et al. Guidelines for management of patients with unruptured intracranial aneurysms. https://pubmed.ncbi.nlm.nih.gov/26089327/
-
Vlak MH, Algra A, Brandenburg R, Rinkel GJ. Prevalence of unruptured intracranial aneurysms. https://pubmed.ncbi.nlm.nih.gov/19542055/
-
Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. https://pubmed.ncbi.nlm.nih.gov/23663953/
-
National Institute of Neurological Disorders and Stroke. Brain Aneurysm Information Page. https://www.ninds.nih.gov/health-information/disorders/cerebral-aneurysms
-
American Stroke Association. Brain Aneurysm and Subarachnoid Hemorrhage Overview. https://www.stroke.org/en/about-stroke/types-of-stroke/hemorrhagic-strokes-bleeds/brain-aneurysm-and-subarachnoid-hemorrhage
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge