Right 5th metacarpal base fracture: presentation, diagnosis, management, outcomes case report
OthersPage Navigation
Abstract
Fractures of the base of the fifth metacarpal, commonly referred to as “reverse Bennett’s fractures,” are relatively frequent injuries of the hand, often resulting from axial loading or direct trauma. These fractures may be associated with carpometacarpal (CMC) joint instability, making early recognition and appropriate management critical to prevent long-term functional impairment. Clinical presentation typically includes pain, swelling, reduced grip strength, and limited range of motion, though subtle fractures may be overlooked on initial evaluation.
We report a case of a 28-year-old male presenting with pain and swelling over the right hand following trauma. Radiographic imaging confirmed a fracture at the base of the fifth metacarpal with minimal displacement. The patient was managed conservatively with immobilization and structured rehabilitation, resulting in satisfactory functional recovery. This case highlights the importance of accurate diagnosis, appropriate imaging, and individualized treatment planning in optimizing outcomes for hand injuries.
Introduction
Fractures of the metacarpals account for approximately 30–40% of all hand fractures, with the fifth metacarpal being the most commonly affected. While neck fractures (commonly termed “boxer’s fractures”) are more prevalent, fractures involving the base of the fifth metacarpal are clinically significant due to their proximity to the carpometacarpal (CMC) joint and potential for joint instability.
The base of the fifth metacarpal articulates with the hamate bone, forming a relatively mobile CMC joint that facilitates grip and hand function. Fractures in this region may extend into the articular surface and can be associated with subluxation or dislocation due to the pull of the extensor carpi ulnaris tendon.
Mechanisms of injury typically include direct trauma, falls onto an outstretched hand, or punching injuries. Early diagnosis is essential, as missed or improperly treated fractures can result in chronic pain, reduced grip strength, and post-traumatic arthritis.
This case report describes a typical presentation of a base of the fifth metacarpal fracture, emphasizing diagnostic considerations, management strategies, and functional outcomes.
Case Report
Patient History
A 28-year-old right-hand dominant male presented to the emergency department with pain and swelling over the ulnar aspect of his right hand following a fall from a motorcycle. The injury occurred when he attempted to break his fall using his right hand, resulting in axial loading of the metacarpals.

The patient reported immediate pain, swelling, and difficulty in gripping objects. There was no history of open wounds, numbness, or tingling sensations. He denied any previous hand injuries or chronic illnesses.
Clinical Examination
On examination, the patient had localized swelling over the dorsoulnar aspect of the right hand. Tenderness was noted at the base of the fifth metacarpal.
Vital signs were stable. Local examination revealed:
- Moderate edema and mild ecchymosis
- Pain on palpation at the fifth metacarpal base
- Reduced grip strength
- Limited range of motion of the little finger
- No rotational deformity
- Intact neurovascular status
There was no evidence of open injury or gross deformity.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
- Fracture of the fifth metacarpal base
- Fifth metacarpal neck fracture (boxer’s fracture)
- Carpometacarpal joint dislocation
- Soft tissue injury (ligament sprain)
- Hamate fracture
The mechanism of injury and localized tenderness raised suspicion for a metacarpal base fracture.
Investigations
Radiological Evaluation
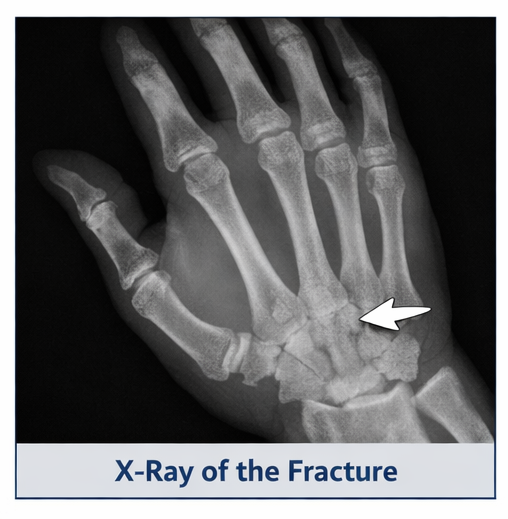
Plain radiographs of the right hand (anteroposterior, oblique, and lateral views) revealed:
- A fracture at the base of the fifth metacarpal
- Minimal displacement
- No significant articular incongruity
- No associated dislocation of the CMC joint
In cases where radiographs are inconclusive, computed tomography (CT) may be utilized to assess articular involvement and fracture complexity. However, in this case, X-rays were sufficient for diagnosis.
Diagnosis
Based on clinical findings and radiographic confirmation, a diagnosis of a minimally displaced fracture of the base of the fifth metacarpal of the right hand was established.
Management and Outcome
Management Strategy
Conservative Treatment
Given the minimal displacement and absence of joint instability, the patient was managed conservatively. Treatment included:
- Immobilization using an ulnar gutter splint

- Positioning the hand in the intrinsic plus position
- Analgesics for pain control
- Ice application to reduce swelling
The patient was advised to avoid weight-bearing and strenuous hand activities.
Rehabilitation
After three weeks of immobilization, gradual mobilization was initiated:
- Passive and active range-of-motion exercises
- Grip strengthening exercises
- Hand therapy to restore function

Physiotherapy played a crucial role in preventing stiffness and improving outcomes.
Follow-Up and Outcome
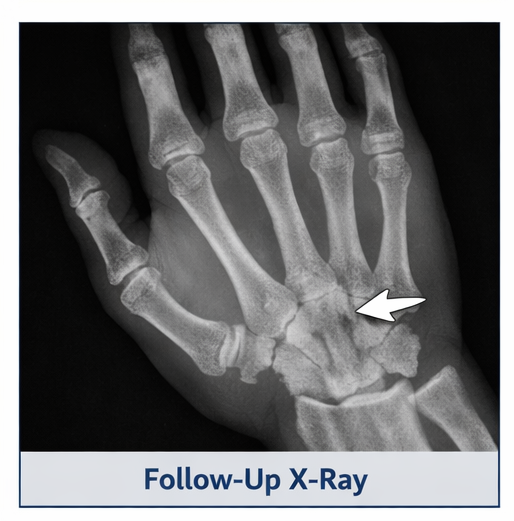
At 4 weeks:
- Pain significantly reduced
- Swelling subsided
- Early callus formation noted on X-ray
At 8 weeks:
- Full range of motion achieved
- Grip strength improved
- Radiological evidence of fracture healing
At 12 weeks:
- Patient returned to normal activities
- No residual pain or functional limitation
- No evidence of malunion or instability
The patient achieved complete functional recovery without complications.

Discussion
Fractures of the base of the fifth metacarpal require careful evaluation due to their potential involvement of the carpometacarpal joint. Unlike neck fractures, base fractures may compromise joint stability and lead to long-term dysfunction if not properly managed.
Mechanism and Pathophysiology
These fractures often result from axial loading or direct trauma. The deforming force of the extensor carpi ulnaris tendon may cause dorsal displacement, particularly in unstable fractures.
Diagnostic Challenges
Diagnosis may be challenging due to:
- Subtle radiographic findings
- Overlapping structures on X-ray
- Misinterpretation as soft tissue injury
Multiple radiographic views are essential. CT imaging is recommended in complex or intra-articular fractures.
Treatment Considerations
Management depends on:
- Degree of displacement
- Articular involvement
- Stability of the CMC joint
Conservative treatment is appropriate for:
- Minimally displaced fractures
- Stable joints
Surgical intervention (e.g., K-wire fixation or open reduction) is indicated for:
- Significant displacement
- Joint incongruity
- Instability
Complications
Potential complications include:
- Malunion
- Reduced grip strength
- Chronic pain
- Post-traumatic arthritis
- Joint stiffness
Early mobilization and rehabilitation are critical in minimizing these risks.
Prognosis
With appropriate management, most patients achieve excellent outcomes. Stable fractures treated conservatively typically heal within 6–8 weeks, with full functional recovery.
Conclusion
Fracture of the base of the fifth metacarpal is a clinically significant injury that requires prompt diagnosis and appropriate management. This case demonstrates that conservative treatment with immobilization and structured rehabilitation can lead to excellent outcomes in minimally displaced fractures.
Accurate imaging, careful assessment of joint stability, and adherence to rehabilitation protocols are essential in preventing long-term complications and ensuring optimal hand function. Early intervention and patient compliance remain key determinants of successful recovery.
References
- American Academy of Orthopaedic Surgeons. (n.d.). Metacarpal fractures. https://www.assh.org/handcare/condition/metacarpal-fractures
- Eiff, M. P., Hatch, R. L., & Calmbach, W. L. (2012). Fracture management for primary care (3rd ed.). American Academy of Family Physicians. https://www.aafp.org/pubs/afp/issues/2012/0415/p805.html
- Giddins, G. (2015). The non-operative management of hand fractures. Journal of Hand Surgery (European Volume), 40(1), 33–41. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4444924/
- Jupiter, J. B., & Hastings, H. (2008). Management of metacarpal fractures. Journal of Orthopaedic Trauma, 22(6), 1–6. https://journals.lww.com/jorthotrauma/Abstract/2008/06000/Management_of_Metacarpal_Fractures.6.aspx
- National Center for Biotechnology Information. (2023). Metacarpal fractures. In StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK551532/
- National Center for Biotechnology Information. (2023). Hand fractures. In StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK470428/
- Orthobullets. (n.d.). Metacarpal fractures. https://www.orthobullets.com/hand/6037/metacarpal-fractures
- Radiopaedia. (n.d.). Metacarpal fractures. https://radiopaedia.org/articles/metacarpal-fractures
- Elsevier. (n.d.). Metacarpal fracture overview. https://www.sciencedirect.com/topics/medicine-and-dentistry/metacarpal-fracture
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge