Amoebiasis (Entamoeba histolytica): Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Amoebiasis is a protozoal infection of the gastrointestinal tract caused by Entamoeba histolytica infection. It is highly prevalent in developing countries and is a significant cause of morbidity and mortality, particularly due to its extraintestinal manifestations such as amoebic liver abscess. The clinical presentation ranges from asymptomatic colonization to severe invasive disease.
We report the case of a 35-year-old male who presented with fever, right upper quadrant abdominal pain, and diarrhea. Imaging revealed a solitary liver abscess, and serological testing confirmed amoebiasis. The patient was managed with antiparasitic therapy, resulting in marked clinical and radiological improvement.
This case highlights the importance of early diagnosis, appropriate imaging, and timely medical therapy in improving outcomes and preventing complications.
Introduction
Amoebiasis is caused by ingestion of cysts of Entamoeba histolytica infection, typically through contaminated food or water. Following ingestion, cysts release trophozoites in the intestine, which can invade the colonic mucosa or disseminate via the portal circulation to the liver and other organs.
The disease is endemic in regions with poor sanitation, overcrowding, and limited access to clean water. It remains a leading cause of parasitic infections globally and contributes significantly to gastrointestinal and hepatic morbidity.
Clinical manifestations are variable and include:
- Asymptomatic infection
- Amoebic colitis (diarrhea, dysentery)
- Extraintestinal disease (most commonly liver abscess)
The progression of disease depends on host immunity, parasite virulence, and environmental factors. Early diagnosis and treatment are crucial to reduce complications and transmission.
Case Report
Patient History
A 35-year-old male presented to the emergency department with:
- Fever for 10 days, intermittent and associated with chills
- Right upper quadrant abdominal pain, dull and progressively worsening
- Loose stools for 7 days, non-bloody
- Loss of appetite and generalized weakness
There was no history of vomiting, jaundice, or gastrointestinal bleeding. The patient reported frequent consumption of street food and untreated drinking water. He resided in a semi-urban area with suboptimal sanitation.
No prior history of liver disease, diabetes, or immunocompromised state was noted. There was no significant family history.
Clinical Examination
General Examination
- Temperature: 38.7°C
- Pulse: 96/min
- Blood pressure: 110/70 mmHg
- Mild dehydration
Abdominal Examination
- Tenderness in the right hypochondrium
- Mild hepatomegaly
- No guarding or rigidity
Other Systems
- Cardiovascular, respiratory, and neurological examinations were within normal limits
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation, the following were considered:
- Amoebic liver abscess
- Pyogenic liver abscess
- Acute viral hepatitis
- Cholecystitis
The combination of fever, localized abdominal pain, and epidemiological risk factors strongly suggested an infectious etiology.
Investigations
Laboratory Findings
- Hemoglobin: Mild anemia
- Total leukocyte count: Elevated (leukocytosis)
- ESR and CRP: Elevated
- Liver function tests: Mild elevation of alkaline phosphatase
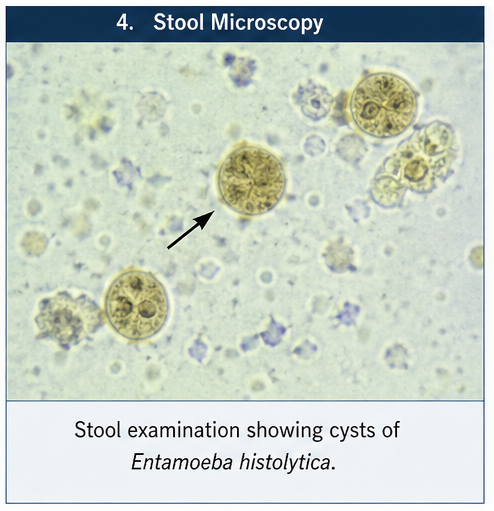
Stool Examination
- Presence of cysts of Entamoeba histolytica infection
Serological Tests
- Amoebic antibody test: Positive

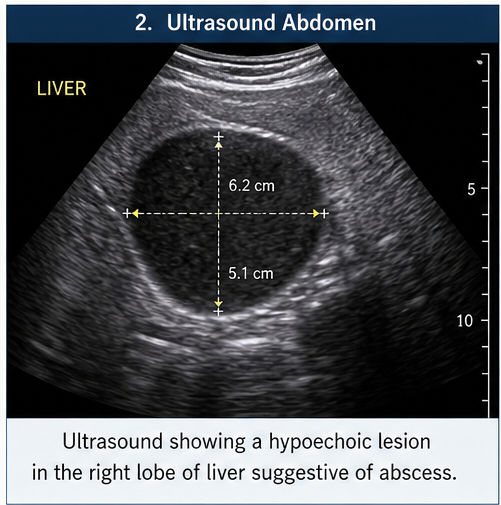
Imaging
Ultrasound Abdomen
- Hypoechoic lesion in the right lobe of the liver
CT Scan Abdomen
- Single well-defined abscess measuring 6 × 5 cm
- Peripheral rim enhancement
- No evidence of rupture
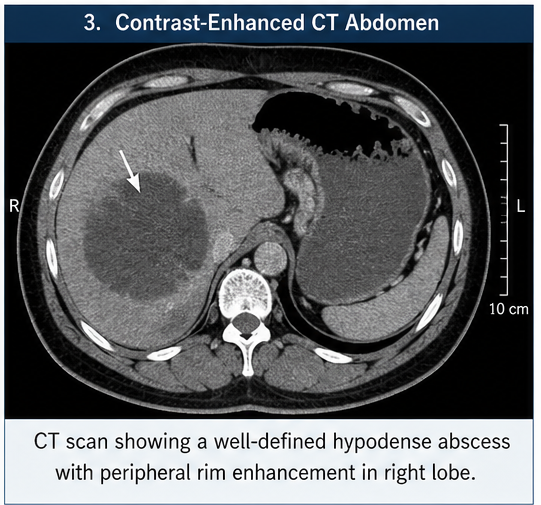
Findings were consistent with amoebic liver abscess.
Diagnosis
A diagnosis of amoebic liver abscess secondary to Amoebiasis was established based on a comprehensive correlation of clinical, radiological, and laboratory findings. The patient’s presentation with fever, right upper quadrant pain, and gastrointestinal symptoms, along with epidemiological risk factors such as exposure to contaminated food and water, raised a strong initial suspicion. Imaging studies, including ultrasound and contrast-enhanced CT, demonstrated a characteristic hepatic abscess with supportive features. This was further substantiated by positive serological testing for Entamoeba histolytica infection antibodies, thereby confirming the diagnosis and excluding other potential differentials such as pyogenic abscess or malignancy.
Management and Outcome
Management Strategy
Treatment was guided by:
- Size and location of the abscess
- Severity of symptoms
- Risk of complications
Medical Management
Antiparasitic Therapy
- Metronidazole administered at 750 mg three times daily for 10 days
Luminal Therapy
- Diloxanide furoate initiated after completion of metronidazole to eradicate intestinal cysts
Supportive Care
- Intravenous fluids
- Antipyretics
- Nutritional support
Clinical Course
During hospitalization:
- Fever subsided within 72 hours
- Abdominal pain gradually improved
- No signs of abscess rupture or complications
Follow-Up
At 2 Weeks
- Significant symptomatic relief
- Improved appetite
At 1 Month
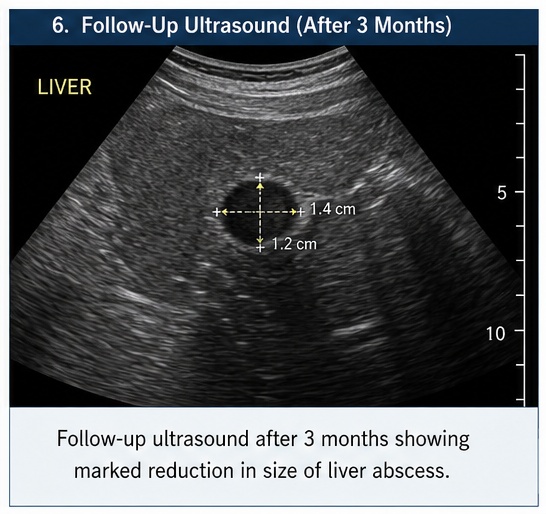
- Ultrasound showed reduction in abscess size
At 3 Months
- Near-complete resolution of abscess
- No recurrence of symptoms
The patient resumed normal activities with good compliance to therapy.
Discussion
Pathophysiology
Amoebiasis results from ingestion of cysts of Entamoeba histolytica infection. These cysts release trophozoites that adhere to and invade the intestinal mucosa, causing tissue destruction.
In some cases, trophozoites enter the portal circulation and localize in the liver, leading to abscess formation. The characteristic “anchovy sauce” pus is due to necrotic hepatocytes rather than true purulence.
Epidemiology
- Highly prevalent in tropical and subtropical regions
- Common in areas with poor sanitation
- Significant cause of liver abscess in developing countries
- Higher incidence in adult males
Clinical Manifestations
Intestinal Amoebiasis
- Diarrhea
- Dysentery
- Abdominal pain
Extraintestinal Amoebiasis
- Fever
- Right upper quadrant pain
- Hepatomegaly
- Weight loss
Diagnostic Considerations
Diagnosis is based on:
- Clinical suspicion
- Stool microscopy (limited sensitivity)
- Serology (high sensitivity in liver abscess)
- Imaging (ultrasound/CT)
Typical imaging features include:
- Hypoechoic liver lesion
- Peripheral enhancement
- Solitary abscess in right lobe
Treatment Considerations
First-Line Therapy
- Metronidazole
Alternative Agents
- Tinidazole
Luminal Agents
- Diloxanide furoate
- Paromomycin
Intervention
- Percutaneous drainage (if large, >10 cm, or non-responsive)
Complications
- Abscess rupture into peritoneal or pleural cavity
- Secondary bacterial infection
- Chronic liver damage
- Recurrence
Prognosis
The prognosis is favorable with early diagnosis and treatment. Delayed intervention may result in significant morbidity.
Factors affecting outcomes:
- Size and number of abscesses
- Timeliness of therapy
- Patient compliance
- Presence of complications
Conclusion
Amoebiasis remains a major public health concern, particularly in endemic regions. Amoebic liver abscess is a serious but treatable complication that requires a high index of clinical suspicion.
This case highlights the importance of integrating clinical history, epidemiological factors, and imaging findings for accurate diagnosis. Early initiation of antiparasitic therapy, followed by luminal agents, plays a crucial role in achieving favorable outcomes.
Preventive strategies such as improved sanitation, access to clean drinking water, and public health education are essential to reduce disease burden.
Timely diagnosis, individualized treatment, and regular follow-up are key to preventing complications and ensuring complete recovery.
References
- Stanley, S. L. (2003). Amoebiasis. The Lancet. https://pubmed.ncbi.nlm.nih.gov/12711473/
- Haque, R., et al. (2003). Amebiasis. New England Journal of Medicine. https://pubmed.ncbi.nlm.nih.gov/12867608/
- Shirley, D. A., et al. (2018). Amebiasis. Clinical Microbiology Reviews. https://pubmed.ncbi.nlm.nih.gov/29386229/
- Petri, W. A., et al. (2000). Enteric amoebiasis. New England Journal of Medicine. https://pubmed.ncbi.nlm.nih.gov/10660346/
- World Health Organization. Amoebiasis Fact Sheet. https://www.who.int/health-topics/amoebiasis
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge