Central Retinal Artery Occlusion (CRAO): Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Central retinal artery occlusion (CRAO) is an ophthalmic emergency characterized by sudden, painless, and severe vision loss due to acute interruption of retinal arterial blood flow. It is often associated with embolic or thrombotic events and shares risk factors with systemic vascular diseases such as hypertension, diabetes mellitus, and atherosclerosis. The retina is highly sensitive to ischemia, and irreversible damage can occur within a short time window. Diagnosis is primarily clinical, supported by fundoscopic findings and imaging modalities such as optical coherence tomography (OCT) and fluorescein angiography. Despite various treatment attempts, visual prognosis remains poor in most patients. This case report highlights the clinical presentation, diagnostic approach, management, and outcome of CRAO in a middle-aged patient.
Introduction
Central retinal artery occlusion represents the ocular equivalent of an ischemic stroke and requires immediate recognition and intervention. The central retinal artery, a branch of the ophthalmic artery, supplies the inner retinal layers. Any obstruction in this artery results in rapid retinal ischemia and subsequent vision loss.
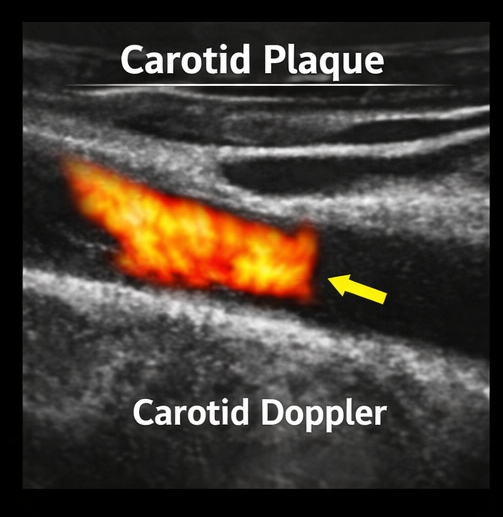
CRAO most commonly occurs due to emboli originating from atherosclerotic plaques in the carotid arteries or cardiac sources such as atrial fibrillation. Less frequently, it may result from thrombosis, vasculitis, or hypercoagulable states. The condition predominantly affects older adults with underlying vascular risk factors.
Clinically, CRAO presents as sudden, painless, unilateral vision loss, often described as a curtain descending over the visual field. Prompt diagnosis is critical, although the therapeutic window for meaningful visual recovery is extremely narrow.
Case Report
Patient History
A 60-year-old male presented to the emergency department with sudden onset of vision loss in the left eye for approximately 3 hours. The loss of vision was painless and complete, with no preceding trauma, redness, or discharge.
The patient had a known history of hypertension, type 2 diabetes mellitus, and hyperlipidemia for over 10 years. He was a chronic smoker with poor adherence to medications. There was no prior history of ocular disease or similar episodes.
Clinical Examination
On examination, the patient was hemodynamically stable.
Ophthalmic findings included:
- Visual acuity: Hand movements in the left eye; normal in the right eye
- Relative afferent pupillary defect (RAPD) in the affected eye
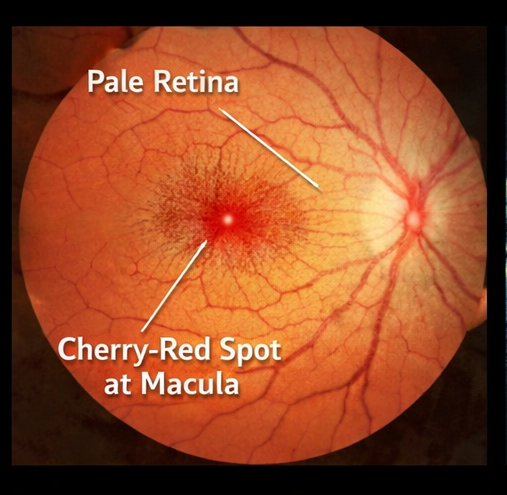
Fundus examination revealed:
- Diffuse retinal whitening
- A prominent cherry-red spot at the macula
- Attenuated and narrowed retinal arteries
Anterior segment examination was normal, and intraocular pressure was within normal limits.
Clinical Evaluation
Differential Diagnosis
The differential diagnoses considered included:
- Central retinal artery occlusion
- Central retinal vein occlusion
- Retinal detachment
- Optic neuritis
- Anterior ischemic optic neuropathy
The classic fundoscopic findings and sudden painless vision loss strongly indicated CRAO.
Investigations
Laboratory Findings
- Elevated fasting blood glucose levels
- Increased serum cholesterol and triglycerides
- Normal complete blood count except mild leukocytosis
Ophthalmic Imaging
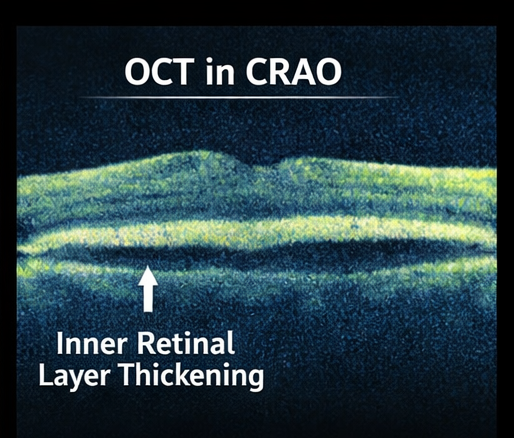
- Optical Coherence Tomography (OCT): Hyperreflectivity and thickening of inner retinal layers
- Fundus Fluorescein Angiography: Delayed arterial filling and reduced retinal perfusion
Systemic Evaluation
- Carotid Doppler ultrasound: Atherosclerotic plaque in the internal carotid artery
- Electrocardiogram (ECG): No arrhythmia detected
- Echocardiography: No significant cardiac source of emboli
Diagnosis
Based on clinical presentation and supporting investigations, the diagnosis was confirmed as:
Acute Central Retinal Artery Occlusion
Management and Outcome
Initial Management
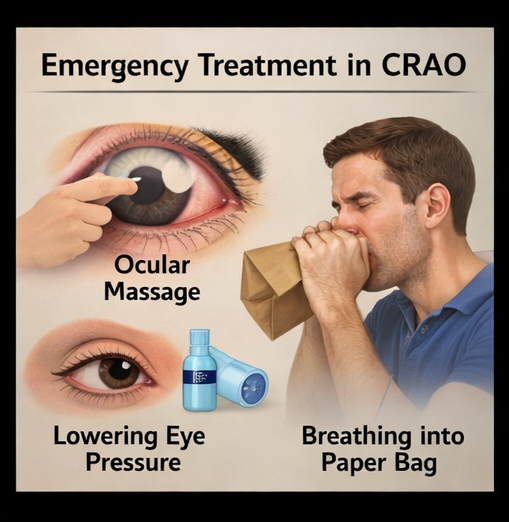
Immediate treatment was initiated in an attempt to restore retinal perfusion:
- Ocular massage to dislodge embolus
- Reduction of intraocular pressure using topical beta-blockers and systemic agents
- Administration of carbon dioxide via rebreathing technique to induce vasodilation
Medical Management
- Antiplatelet therapy initiated
- Statins prescribed for lipid control
- Optimization of blood pressure and glycemic status
Follow-Up
At 1 week:
- No significant improvement in vision
At 1 month:
- Persistent severe visual impairment
- Fundus showed resolving edema
At 3 months:
- Optic disc pallor indicating optic atrophy
- Permanent loss of central vision
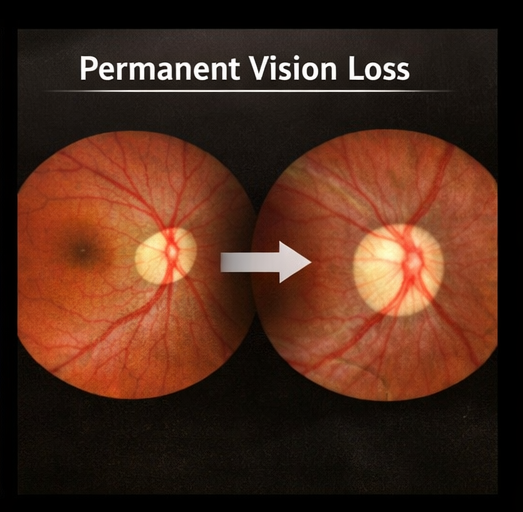
Outcome
The patient experienced:
- Irreversible vision loss in the affected eye
- Stabilization of systemic risk factors with medical therapy
- No recurrence or involvement of the contralateral eye
Discussion
Central retinal artery occlusion is a devastating ocular condition with limited treatment options and poor visual prognosis. The retina has one of the highest metabolic demands in the body, making it extremely vulnerable to ischemia. Experimental studies suggest that irreversible damage can occur within 90–120 minutes of occlusion.
The most common etiology is embolic occlusion from carotid artery atherosclerosis or cardiac sources. Risk factors such as hypertension, diabetes, smoking, and hyperlipidemia significantly increase the likelihood of occurrence.
The hallmark clinical feature is sudden, painless, unilateral vision loss. Fundoscopic examination typically reveals retinal whitening due to ischemia and a cherry-red spot at the fovea, where the underlying choroidal circulation remains intact.
Diagnosis is largely clinical but is supported by imaging modalities. OCT findings reflect ischemic damage to inner retinal layers, while fluorescein angiography demonstrates delayed or absent arterial filling.
Management remains controversial and largely ineffective in restoring vision. Conventional approaches such as ocular massage, reduction of intraocular pressure, and vasodilation techniques are often attempted but lack strong evidence. Recent studies have explored thrombolytic therapy; however, its use remains limited due to potential risks and lack of consensus.
Importantly, CRAO is considered a manifestation of systemic vascular disease and is associated with an increased risk of stroke and cardiovascular events. Therefore, comprehensive systemic evaluation is essential.
Complications include:
- Permanent vision loss
- Optic atrophy
- Neovascularization (rare)
- Increased risk of cerebrovascular events
Preventive strategies focus on aggressive management of cardiovascular risk factors and lifestyle modifications such as smoking cessation.
Conclusion
Central retinal artery occlusion is a true ophthalmic emergency that requires rapid diagnosis and immediate intervention. Despite timely management, visual outcomes are often poor due to the rapid onset of irreversible retinal ischemia. This case highlights the importance of early recognition, prompt referral, and systemic evaluation to reduce the risk of further vascular events. Clinicians should maintain a high index of suspicion in patients presenting with sudden painless vision loss, particularly those with underlying vascular risk factors.
References
- Hayreh SS, Zimmerman MB, Kimura A, Sanon A. Central retinal artery occlusion. https://pubmed.ncbi.nlm.nih.gov/16678504/
- Varma DD, Cugati S, Lee AW, Chen CS. A review of central retinal artery occlusion: clinical presentation and management. https://pubmed.ncbi.nlm.nih.gov/24068003/
- Schrag M, Youn T, Schindler J, et al. Intravenous fibrinolytic therapy in central retinal artery occlusion. https://pubmed.ncbi.nlm.nih.gov/26642484/
- Mac Grory B, Schrag M, Biousse V, et al. Management of central retinal artery occlusion: A scientific statement. https://pubmed.ncbi.nlm.nih.gov/33626989/
- Biousse V, Nahab F, Newman NJ. Management of acute retinal ischemia. https://pubmed.ncbi.nlm.nih.gov/21282583/
- Fraser SG, Adams W. Interventions for acute non-arteritic central retinal artery occlusion. https://pubmed.ncbi.nlm.nih.gov/24395564/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge