Folliculitis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Folliculitis is a common inflammatory disorder involving the hair follicles, frequently caused by bacterial, fungal, viral, or mechanical factors. It commonly presents as erythematous follicular papules and pustules and may affect any hair-bearing region of the body. Although superficial folliculitis is often self-limiting, recurrent or untreated cases can lead to deeper infection, scarring, and cosmetic concerns.
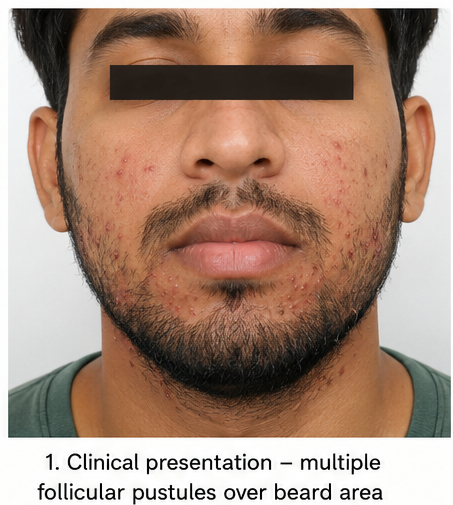
We present the case of a 28-year-old male who developed painful pustular lesions over the beard region and anterior neck following frequent shaving and excessive sweating. Clinical examination revealed multiple follicle-centered papules and pustules with perifollicular erythema, suggestive of bacterial folliculitis. Microbiological evaluation supported superficial Staphylococcus aureus infection. The patient was treated with topical and systemic antimicrobial therapy along with hygiene modification, resulting in complete clinical resolution without recurrence.
This case highlights the importance of early recognition, identification of precipitating factors, and appropriate antimicrobial management in preventing complications associated with folliculitis.
Introduction
Folliculitis refers to inflammation or infection of the hair follicles and is one of the most frequently encountered dermatological conditions in clinical practice. The disorder may involve superficial or deep portions of the follicular unit and can arise from infectious or noninfectious etiologies. Infectious folliculitis is most commonly caused by Staphylococcus aureus, although fungal organisms such as Malassezia and dermatophytes may also be implicated.
Clinically, folliculitis presents as small erythematous papules or pustules centered around hair follicles. The lesions may be associated with itching, tenderness, burning sensation, or mild pain. Commonly affected areas include the scalp, beard area, axillae, buttocks, chest, and thighs.
Several predisposing factors contribute to folliculitis, including excessive sweating, poor hygiene, friction from tight clothing, occlusion, obesity, diabetes mellitus, prolonged antibiotic use, immunosuppression, and repeated shaving. Mechanical trauma caused by shaving often leads to disruption of the follicular epithelium, increasing susceptibility to bacterial invasion.
Although superficial folliculitis usually resolves with conservative management, recurrent or severe disease may progress to furunculosis, cellulitis, or permanent scarring. Accurate diagnosis and timely treatment are therefore essential for optimal outcomes.
Case Report
Patient History
A 28-year-old male presented to the dermatology outpatient department with complaints of multiple painful pustular lesions over the beard area and anterior neck for the past seven days. The lesions initially appeared as small red bumps and progressively developed into pustules associated with mild itching and burning sensation.
The patient reported frequent shaving using a reusable razor and excessive sweating due to outdoor occupational activity. He also admitted to occasional sharing of personal grooming equipment with coworkers.
There was no history of fever, weight loss, diabetes mellitus, immunosuppressive illness, or previous recurrent skin infections. The patient denied any recent use of systemic corticosteroids or long-term antibiotics.
Family history was unremarkable for chronic dermatological disorders or autoimmune diseases.
Clinical Examination
General Examination
The patient was conscious, alert, and hemodynamically stable. Vital signs were within normal limits. No pallor, cyanosis, clubbing, or lymphadenopathy was noted.
Dermatological Examination
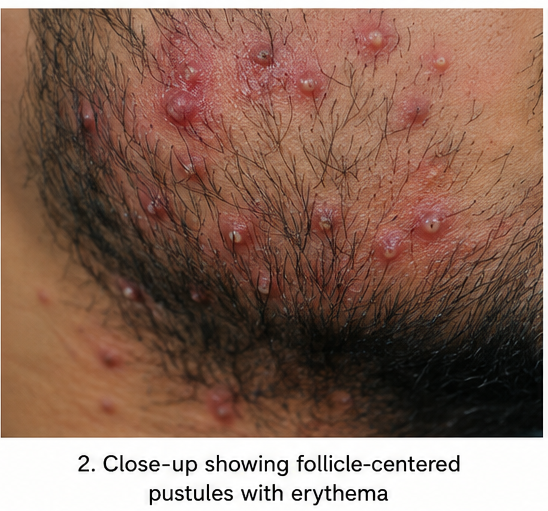
Cutaneous examination revealed multiple follicle-centered erythematous papules and pustules distributed over the beard region and anterior neck. Several lesions demonstrated surrounding perifollicular erythema and mild tenderness on palpation.

No fluctuation, abscess formation, sinus tract, or necrosis was observed. There was no associated alopecia or scarring. The surrounding skin showed mild irritation consistent with repeated shaving trauma.
No lesions were identified over the scalp, trunk, axillae, or extremities.
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation, the following differential diagnoses were considered:
- Bacterial folliculitis (most likely)
- Pseudofolliculitis barbae
- Fungal folliculitis
- Acne vulgaris
- Furunculosis
The presence of follicular pustules with perifollicular erythema and recent shaving history strongly favored superficial bacterial folliculitis.
The absence of comedones excluded acne vulgaris, while the lack of deep nodules or abscesses made furunculosis less likely.
Investigations
Microbiological Evaluation
Pus obtained from one of the pustular lesions was sent for Gram staining and culture sensitivity testing.
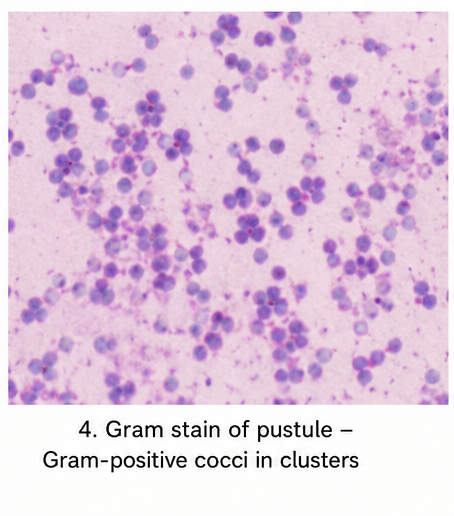
Gram Staining
Demonstrated gram-positive cocci arranged in clusters.
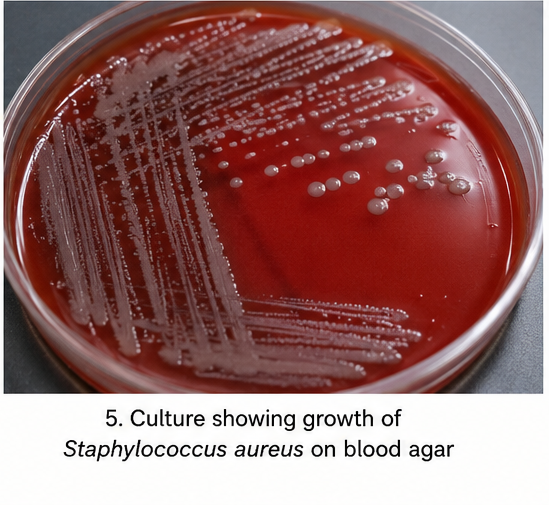
Culture Findings
Culture revealed growth of Staphylococcus aureus sensitive to cephalexin and mupirocin.
Laboratory Investigations
Routine laboratory investigations were performed to assess systemic status:
- Complete blood count: Mild leukocytosis
- Blood glucose levels: Within normal limits
- Renal function tests: Normal
- Liver function tests: Normal
- HIV screening: Negative
These findings supported localized bacterial infection without systemic involvement.
Diagnosis
A provisional diagnosis of superficial bacterial folliculitis involving the beard region was established based on clinical findings and microbiological confirmation.
The characteristic follicular pustules, recent shaving-related trauma, and isolation of Staphylococcus aureus strongly supported the diagnosis.
The absence of fungal elements, nodulocystic lesions, or chronic relapsing disease helped exclude fungal folliculitis and hidradenitis suppurativa.
Management and Outcome
Management Strategy
The treatment plan focused on:
- Eradication of bacterial infection
- Reduction of local inflammation
- Prevention of recurrence
- Improvement of hygiene practices
Medical Management
The patient was initiated on oral cephalexin therapy for seven days along with topical mupirocin ointment applied twice daily over affected areas.
A mild antiseptic cleanser containing chlorhexidine was advised for daily skin cleansing.
The patient was counseled to avoid:
- Reusing razors
- Sharing grooming equipment
- Excessive friction over affected areas
- Close shaving until complete resolution
Warm compresses were recommended to reduce discomfort and facilitate drainage of superficial pustules.
Post-Treatment Course
The patient showed significant clinical improvement within one week of therapy. Pain and erythema reduced substantially, and no new lesions appeared.
By the end of two weeks, most pustules had resolved completely without pigmentation or scarring.
Follow-Up
At 2 Weeks
Marked reduction in inflammatory lesions was observed. Minimal residual erythema persisted over previously affected follicles.
No abscess formation or secondary infection was identified.
At 1 Month
Complete resolution of follicular lesions was noted. The patient remained asymptomatic and resumed shaving using hygienic precautions.
No recurrent pustules were observed.
At 3 Months
The patient maintained healthy skin without recurrence. Compliance with hygiene recommendations and avoidance of razor sharing contributed to sustained improvement.

Discussion
Pathophysiology
Folliculitis develops when hair follicles become inflamed due to microbial invasion, occlusion, friction, or chemical irritation. In bacterial folliculitis, disruption of the follicular epithelium allows colonizing organisms, particularly Staphylococcus aureus, to invade superficial follicular structures.
Local inflammation results in neutrophilic infiltration, pustule formation, and surrounding erythema. Repeated trauma from shaving further damages the follicular barrier and promotes bacterial proliferation.
Etiology and Risk Factors
Common causes and risk factors for folliculitis include:
- Staphylococcus aureus infection
- Excessive sweating
- Occlusive clothing
- Frequent shaving
- Poor hygiene
- Obesity
- Diabetes mellitus
- Immunosuppression
- Prolonged antibiotic use
Hot tub exposure may predispose individuals to Pseudomonas folliculitis, while fungal organisms can cause chronic or recurrent disease in immunocompromised patients.
Epidemiology
Folliculitis affects individuals of all age groups and is among the most common superficial bacterial skin infections. Males are more frequently affected in the beard region due to regular shaving practices.
Occupational heat exposure and humid climates further increase disease prevalence.
Clinical Manifestations
Clinical presentation varies depending on severity and depth of follicular involvement.
Common manifestations include:
- Follicular papules
- Pustules
- Erythema
- Mild pain or tenderness
- Burning sensation
- Itching
Deep follicular involvement may lead to furuncles, carbuncles, cellulitis, or scarring.
Diagnostic Considerations
Diagnosis is primarily clinical and supported by microbiological testing when necessary.
Important diagnostic methods include:
- Clinical dermatological examination
- Gram staining
- Bacterial culture and sensitivity
- Fungal microscopy in suspected fungal cases
- Dermoscopy in recurrent disease
Microbiological evaluation is especially important in recurrent or treatment-resistant folliculitis.
Treatment Considerations
Conservative Measures
Mild folliculitis may improve with:
- Improved hygiene
- Warm compresses
- Avoidance of friction
- Temporary discontinuation of shaving
Pharmacological Therapy
Treatment options depend on severity and etiology.
Topical Therapy
- Mupirocin
- Clindamycin
- Fusidic acid
- Benzoyl peroxide preparations
Systemic Therapy
Oral antibiotics may be required in extensive disease, including:
- Cephalexin
- Dicloxacillin
- Doxycycline
- Clindamycin
Fungal folliculitis may require antifungal therapy such as itraconazole or fluconazole.
Emerging Therapies
Recent advances include:
- Laser hair reduction for recurrent pseudofolliculitis
- Photodynamic therapy
- Antimicrobial peptide-based treatments
- AI-assisted dermatological imaging
Complications
Untreated folliculitis can result in:
- Furunculosis
- Cellulitis
- Abscess formation
- Post-inflammatory hyperpigmentation
- Permanent scarring
- Secondary systemic infection
Early treatment significantly reduces complication risk.
Prognosis
The prognosis of superficial bacterial folliculitis is generally excellent with appropriate therapy and hygiene measures.
Recurrence is common when underlying risk factors persist, particularly repeated shaving trauma or poor sanitation practices.
Prompt diagnosis and targeted antimicrobial treatment usually result in complete recovery without long-term sequelae.
Conclusion
Folliculitis is a common inflammatory and infectious disorder of hair follicles with diverse etiologies and clinical presentations. This case demonstrates the importance of recognizing shaving-related bacterial folliculitis and initiating timely antimicrobial therapy.
Appropriate microbiological evaluation, targeted treatment, and patient education regarding hygiene practices remain essential components of successful management.
Early intervention helps prevent progression to deeper infection, recurrence, and permanent scarring while improving overall patient quality of life.
References
- Otberg N, Kang H, Alzolibani AA, Shapiro J. Folliculitis decalvans. https://pubmed.ncbi.nlm.nih.gov/20883975/
- StatPearls. Folliculitis Overview. https://www.ncbi.nlm.nih.gov/books/NBK547754/
- Bolognia JL, et al. Dermatology – Bacterial skin infections. https://pubmed.ncbi.nlm.nih.gov/29489298/
- American Academy of Dermatology. Folliculitis: Diagnosis and treatment. https://www.aad.org/public/diseases/a-z/folliculitis-treatment
- Craft N, Fox LP. Management of superficial bacterial folliculitis. https://pubmed.ncbi.nlm.nih.gov/25441466/
- DermNet NZ. Folliculitis. https://dermnetnz.org/topics/folliculitis
- Luelmo-Aguilar J, et al. Folliculitis and perifolliculitis. https://pubmed.ncbi.nlm.nih.gov/10566568/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge