Corneal Ulcer: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Corneal ulcer is a potentially sight-threatening ocular condition characterized by disruption of the corneal epithelium with underlying stromal inflammation and necrosis. It is most commonly caused by microbial infections, including bacterial, fungal, viral, or protozoal pathogens, often following trauma, contact lens use, or ocular surface disease. Patients typically present with pain, redness, photophobia, blurred vision, and discharge. Prompt diagnosis through clinical examination and microbiological investigations is essential to prevent complications such as corneal scarring, perforation, or vision loss.
This case report describes a middle-aged male presenting with a unilateral corneal ulcer secondary to bacterial infection following minor ocular trauma, highlighting the diagnostic approach, therapeutic management, and favorable clinical outcome with timely intervention.
Introduction
Corneal ulcer, also referred to as infectious keratitis, is a serious ophthalmic emergency that requires immediate attention. It involves epithelial defect with stromal infiltration, often accompanied by inflammation of surrounding corneal tissue. The condition can rapidly progress and result in permanent visual impairment if not managed appropriately.
The etiology of corneal ulcers varies geographically and is influenced by environmental, occupational, and socioeconomic factors. In developing regions, trauma with vegetative matter and fungal infections are more prevalent, whereas in urban settings, contact lens-associated bacterial keratitis is common.
Risk factors include ocular trauma, improper contact lens hygiene, dry eye disease, eyelid abnormalities, and immunocompromised states. Early clinical recognition and targeted antimicrobial therapy are crucial in preventing adverse outcomes.
Case Report
Patient History
A 42-year-old male presented to the ophthalmology outpatient department with complaints of pain, redness, and decreased vision in the right eye for 5 days. The patient reported a history of minor trauma to the eye with a foreign body (dust particle) while working outdoors.
Symptoms included:
- Severe ocular pain
- Excessive tearing
- Photophobia
- Blurred vision
- Mucopurulent discharge
There was no history of contact lens use, previous ocular surgery, or chronic eye disease. The patient was otherwise healthy, with no known systemic illnesses such as diabetes or immunodeficiency.
Clinical Examination
On ocular examination:
Visual Acuity:
- Right eye: 6/36
- Left eye: 6/6
Slit-Lamp Examination (Right Eye):
- Conjunctival congestion
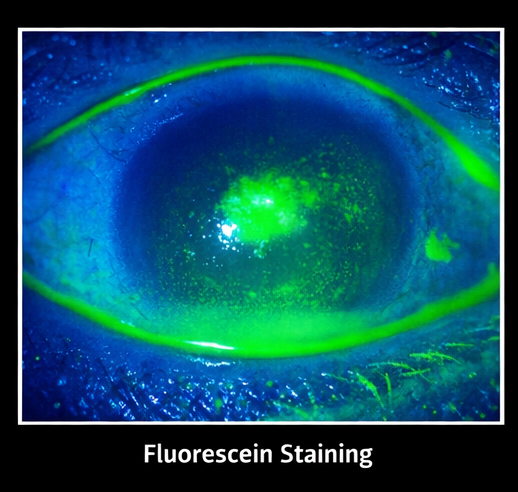
- Corneal epithelial defect with underlying stromal infiltrate
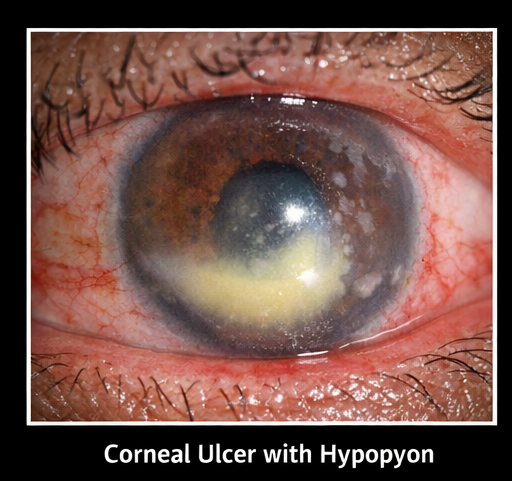
- Ulcer measuring approximately 3 × 2 mm in the central cornea
- Surrounding corneal edema
- Presence of hypopyon (layered white cells in anterior chamber)
- Positive fluorescein staining
Left Eye: Normal
The findings were suggestive of an active infectious corneal ulcer.
Clinical Evaluation
Differential Diagnosis
Based on presentation, the following conditions were considered:
- Bacterial keratitis
- Fungal keratitis
- Herpetic keratitis
- Acanthamoeba keratitis
- Sterile corneal ulcer
The acute onset, purulent discharge, and presence of hypopyon favored a bacterial etiology.
Investigations
Microbiological Evaluation
Corneal scrapings were obtained under aseptic conditions and subjected to:
- Gram staining
- Potassium hydroxide (KOH) mount
- Culture and sensitivity testing
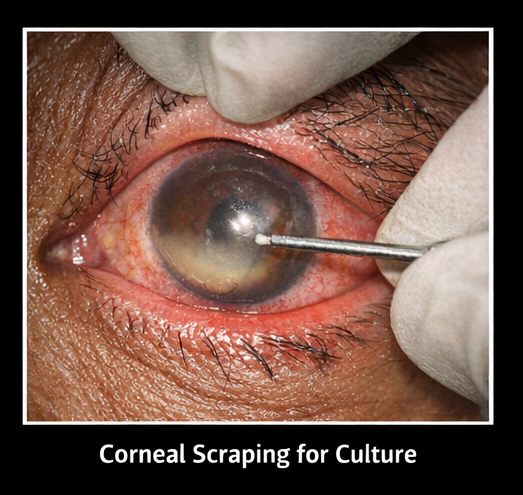
Results:
- Gram stain: Gram-positive cocci
- KOH mount: Negative for fungal elements
- Culture: Growth of Staphylococcus aureus

Additional Tests
- Blood glucose levels: Normal
- Complete blood count: Within normal limits
No systemic risk factors were identified.
Diagnosis
Based on clinical findings and laboratory confirmation, the diagnosis was established as:
Bacterial corneal ulcer (Staphylococcal keratitis) following ocular trauma
Management and Outcome
Initial Management
The patient was treated as an ophthalmic emergency and therapy was initiated immediately.
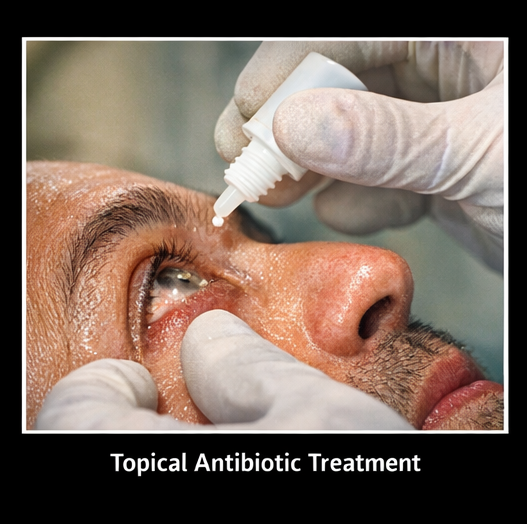
Pharmacological Treatment
- Topical fortified antibiotics:
- Fortified cefazolin (5%)
- Fortified tobramycin (1.3%)
Administered hourly
- Cycloplegic agents:
- Atropine eye drops to relieve ciliary spasm
- Lubricating eye drops:
- Preservative-free artificial tears
- Oral analgesics:
- For pain management
Supportive Measures
- Eye protection
- Avoidance of eye rubbing
- Strict hygiene practices
Follow-Up
At 3 days:
- Reduction in pain and discharge
- Decrease in size of infiltrate
- Hypopyon resolving
At 1 week:
- Significant clinical improvement
- Re-epithelialization of corneal surface
- Improved visual acuity (6/18)
At 3 weeks:
- Complete healing of ulcer
- Residual corneal scar present
- Visual acuity improved to 6/12
Outcome
The patient demonstrated:
- Resolution of infection
- Restoration of corneal integrity
- Significant visual recovery
- No progression to complications such as perforation

Discussion
Corneal ulcer is a major cause of preventable blindness worldwide, particularly in developing countries. The pathogenesis involves microbial invasion following disruption of the corneal epithelium.
Etiology and Risk Factors
Common causes include:
- Bacterial infections (Staphylococcus aureus, Pseudomonas aeruginosa)
- Fungal infections (Fusarium, Aspergillus)
- Viral infections (Herpes simplex virus)
- Protozoal infections (Acanthamoeba)
Predisposing factors:
- Ocular trauma
- Contact lens misuse
- Ocular surface disease
- Immunosuppression
Clinical Features
Patients typically present with:
- Pain and redness
- Decreased vision
- Photophobia
- Discharge
- Corneal opacity
Slit-lamp examination remains the cornerstone of diagnosis.
Diagnostic Approach
- Clinical examination
- Fluorescein staining to detect epithelial defects
- Microbiological analysis for pathogen identification
- Culture and sensitivity testing to guide therapy
Early microbiological diagnosis significantly improves treatment outcomes.
Management Strategies
1. Etiological Treatment
- Targeted antimicrobial therapy based on culture results
2. Empirical Therapy
- Broad-spectrum antibiotics initiated immediately
3. Adjunctive Therapy
- Cycloplegics for pain relief
- Lubricants for epithelial healing
4. Surgical Intervention (if needed)
- Therapeutic keratoplasty in severe or non-responsive cases
Complications
If untreated or inadequately managed, corneal ulcers may lead to:
- Corneal perforation
- Endophthalmitis
- Permanent vision loss
- Dense corneal scarring
Prognosis
The prognosis depends on:
- Size and location of ulcer
- Causative organism
- Timeliness of treatment
Early intervention typically results in favorable outcomes, although central ulcers may leave residual visual impairment due to scarring.
Conclusion
Corneal ulcer is a vision-threatening ophthalmic emergency that demands prompt recognition, accurate diagnosis, and aggressive management to preserve visual function. This case reinforces the critical role of early clinical suspicion, detailed slit-lamp evaluation, and microbiological confirmation in guiding targeted therapy. Timely initiation of appropriate antimicrobial treatment not only halts disease progression but also significantly reduces the risk of complications such as corneal perforation, endophthalmitis, and permanent vision loss.
Equally important is the emphasis on preventive strategies, including the use of protective eyewear in high-risk environments, early and adequate management of ocular trauma, and patient education regarding risk factors such as poor hygiene and delayed treatment-seeking behavior. Strengthening awareness at both patient and primary care levels can facilitate earlier referrals and intervention. With a structured diagnostic approach and adherence to evidence-based management protocols, most cases of corneal ulcer can achieve favorable clinical outcomes, including restoration of corneal integrity and meaningful visual recovery, while minimizing long-term morbidity.
References
- Whitcher JP, Srinivasan M, Upadhyay MP. Corneal blindness: a global perspective. https://pubmed.ncbi.nlm.nih.gov/15172665/
- Ting DSJ, Ho CS, Deshmukh R, Said DG, Dua HS. Infectious keratitis: an update on epidemiology, causative microorganisms, risk factors, and antimicrobial resistance. https://pubmed.ncbi.nlm.nih.gov/31978386/
- Austin A, Lietman T, Rose-Nussbaumer J. Update on the management of infectious keratitis. https://pubmed.ncbi.nlm.nih.gov/28644124/
- Green M, Apel A, Stapleton F. Risk factors and causative organisms in microbial keratitis. https://pubmed.ncbi.nlm.nih.gov/18046230/
- Sharma N, Bagga B, Singhal D, et al. Fungal keratitis: a review of clinical presentations, treatment strategies, and outcomes. https://pubmed.ncbi.nlm.nih.gov/26989956/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge