Pneumocephalus: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Pneumocephalus is a neurological condition characterized by the presence of intracranial air within the cranial cavity. It is most commonly associated with head trauma, neurosurgical procedures, infections, or skull base defects. Clinical presentation varies depending on the volume and location of intracranial air, ranging from mild headache to life-threatening tension pneumocephalus. Early diagnosis is essential, as delayed recognition can lead to neurological deterioration. Diagnostic evaluation primarily relies on imaging modalities such as computed tomography (CT), which is highly sensitive for detecting intracranial air. Management depends on severity and may include conservative measures such as oxygen therapy or surgical intervention in severe cases. This report presents a case of post-traumatic pneumocephalus in a middle-aged patient, highlighting clinical features, diagnostic approach, and successful management.
Introduction
Pneumocephalus refers to the presence of air within the cranial cavity and is an uncommon but clinically significant condition encountered in neurology and neurosurgery. It most frequently occurs following head trauma, especially when there is a breach in the skull or paranasal sinuses allowing air to enter the intracranial space.
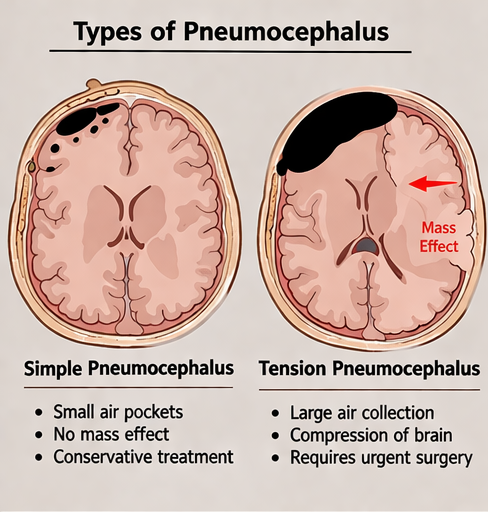
The condition may also arise as a complication of neurosurgical procedures, infections by gas-forming organisms, or spontaneous defects in the skull base. Pneumocephalus can be classified as simple or tension pneumocephalus, with the latter representing a neurosurgical emergency due to increased intracranial pressure and mass effect.
The pathophysiology involves two main mechanisms: the “ball-valve effect,” where air enters but cannot escape, and the “inverted soda bottle effect,” where cerebrospinal fluid (CSF) leakage creates negative pressure, drawing air into the cranial cavity.
Risk factors include:
• Head trauma with skull fractures
• Neurosurgical procedures
• Skull base defects or sinus fractures
• Infections involving the cranial cavity
• Barotrauma
Clinically, patients may present with headache, nausea, dizziness, altered consciousness, or focal neurological deficits. In severe cases, tension pneumocephalus may lead to rapid neurological deterioration.
Early recognition and prompt management are essential to prevent complications and ensure favorable outcomes.
Case Report
Patient History
A 45-year-old male presented to the emergency department following a road traffic accident with complaints of headache and dizziness for two days.
The patient reported:
• Persistent frontal headache
• Episodes of nausea without vomiting
• Mild confusion and reduced concentration
• No history of seizures or loss of consciousness
There was a history of blunt head trauma with impact to the frontal region. No prior neurological illness or surgical history was noted.
Clinical Examination
On general examination, the patient was conscious but mildly disoriented.
Vital signs were stable.
Neurological examination revealed:
• Glasgow Coma Scale (GCS): 14/15
• No focal motor or sensory deficits
• Mild irritability and slowed responses
Local examination showed:
• Bruising over the frontal scalp
• No active bleeding or CSF leak
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
• Concussion or mild traumatic brain injury
• Intracranial hemorrhage
• Pneumocephalus
• Skull fracture with intracranial involvement
• Post-traumatic cerebral edema
Further imaging was planned to confirm the diagnosis.
Investiagtions
Computed Tomography (CT) Scan of Brain
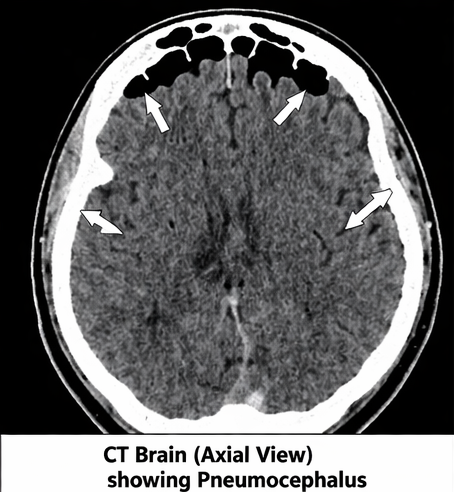
Non-contrast CT scan revealed:
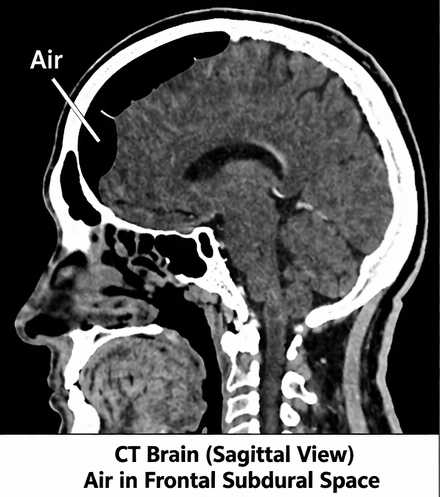
• Presence of air pockets in the frontal intracranial region
• Air accumulation in the subdural space
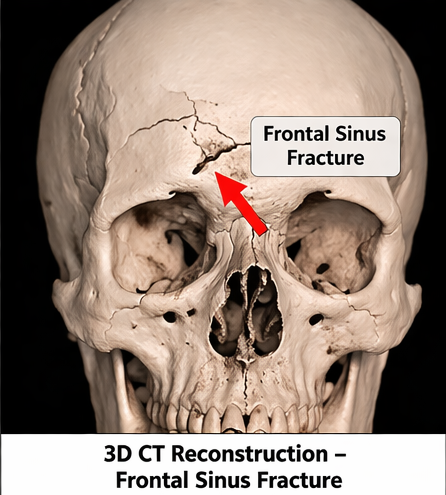
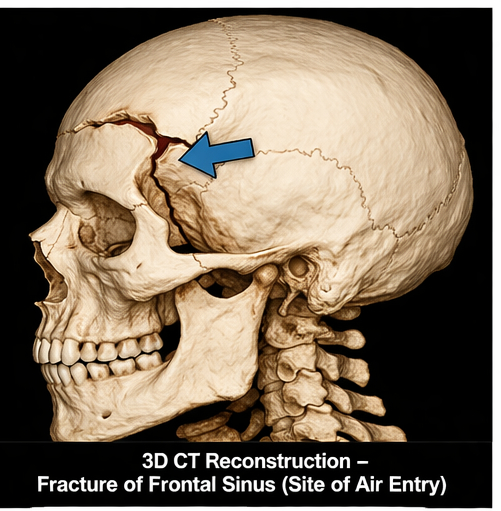
• Fracture of the frontal sinus
• No evidence of intracranial hemorrhage
A characteristic “Mount Fuji sign” was absent, suggesting non-tension pneumocephalus.
Magnetic Resonance Imaging (MRI)
MRI of the brain showed:
• No significant parenchymal injury
• No evidence of abscess or infection
• Confirmation of intracranial air without mass effect
Laboratory Investigations
• Complete blood count: within normal limits
• Electrolytes: normal
• Coagulation profile: normal
Diagnosis
Based on clinical and radiological findings, the patient was diagnosed with:
Post-traumatic pneumocephalus (non-tension type)
Management and Outcome
Initial Management
The patient was admitted for observation and managed conservatively.
Management plan included:
• Bed rest with head elevation
• Administration of high-flow oxygen therapy
• Analgesics for headache
• Avoidance of activities increasing intracranial pressure (e.g., coughing, straining)
Monitoring
The patient was closely monitored for:
• Neurological status
• Signs of increased intracranial pressure
• Development of tension pneumocephalus
Serial neurological examinations were performed.
Clinical Course
Over the next few days:
• Headache gradually subsided
• Orientation improved
• No neurological deterioration was observed
Follow-Up Imaging
Repeat CT scan after five days showed:
• Significant reduction in intracranial air
• No new abnormalities
Outcome
The patient showed steady clinical improvement and was discharged after one week.
At follow-up after one month:
• No residual neurological symptoms
• Complete resolution of pneumocephalus on imaging
• Return to normal daily activities
Discussion
Pneumocephalus is a rare but important condition, most commonly associated with trauma or surgical interventions. The presence of intracranial air can vary from small asymptomatic collections to large volumes causing mass effect.
The frontal region is the most commonly affected site due to its proximity to paranasal sinuses. Fractures involving the frontal sinus or skull base create a pathway for air entry into the cranial cavity.
The distinction between simple and tension pneumocephalus is critical. While simple pneumocephalus is often self-limiting, tension pneumocephalus can lead to rapid neurological deterioration and requires urgent surgical decompression.
CT scan is the gold standard for diagnosis due to its high sensitivity in detecting even small volumes of air. The “Mount Fuji sign” is a classic radiological feature of tension pneumocephalus.
Management depends on severity:
• Conservative management is effective in most cases and includes oxygen therapy and observation
• Surgical intervention is indicated in cases of tension pneumocephalus or persistent air collections
High-flow oxygen therapy accelerates the absorption of intracranial air by increasing the diffusion gradient of nitrogen.
Prognosis is generally favorable in uncomplicated cases, especially when diagnosed early and managed appropriately.
Preventive measures include proper management of head injuries, careful surgical techniques, and early detection of skull base fractures.
Conclusion
Pneumocephalus is a clinically significant condition that requires prompt recognition and appropriate management.
Post-traumatic patients presenting with persistent headache or neurological symptoms should be evaluated with imaging to rule out intracranial air.
CT imaging plays a crucial role in diagnosis and monitoring.
Most cases respond well to conservative treatment, but vigilance is required to identify and manage tension pneumocephalus.
Early diagnosis and appropriate intervention lead to excellent clinical outcomes, as demonstrated in this case.
References
- National Comprehensive Cancer Network (NCCN). Central Nervous System Cancers Guidelines. https://pubmed.ncbi.nlm.nih.gov/30659137/
- Markham JW. Pneumocephalus: report of two cases and review of the literature. https://pubmed.ncbi.nlm.nih.gov/5329331/
- Reasoner DK, et al. Pneumocephalus after neurosurgery: incidence and management. https://pubmed.ncbi.nlm.nih.gov/8098283/
- Ishiwata Y, et al. Subdural tension pneumocephalus following surgery. https://pubmed.ncbi.nlm.nih.gov/7643682/
- Dabdoub CB, et al. Review of pneumocephalus. https://pubmed.ncbi.nlm.nih.gov/24765501/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge