Meningioma: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Meningioma is a common primary intracranial tumor arising from the meningothelial cells of the arachnoid layer. It is typically benign and slow-growing, accounting for approximately one-third of all primary brain tumors. Clinical presentation depends on tumor size and location, ranging from incidental findings to neurological deficits and seizures. Early diagnosis is essential to prevent complications related to mass effect and increased intracranial pressure. Imaging modalities such as magnetic resonance imaging (MRI) and computed tomography (CT) are crucial for diagnosis and surgical planning. Management strategies include observation, surgical resection, and radiotherapy depending on tumor characteristics. This report presents a case of a frontal lobe meningioma in a middle-aged female, highlighting clinical features, diagnostic approach, and successful management.
Introduction
Meningiomas are extra-axial tumors originating from arachnoid cap cells of the meninges. They are generally benign (World Health Organization Grade I), although atypical (Grade II) and malignant (Grade III) variants exist.
These tumors are more commonly observed in females and are often associated with hormonal influences, particularly progesterone receptor expression. Meningiomas can occur at various intracranial sites, with the most frequent locations being the convexity, parasagittal region, sphenoid wing, and skull base.
The pathophysiology involves slow tumor growth leading to compression of adjacent brain structures rather than direct invasion in most cases.
Meningiomas can be classified based on histopathology and location.
Risk factors include:
• Female gender
• Increasing age
• Prior cranial irradiation
• Genetic conditions such as neurofibromatosis type 2
• Hormonal influences
Clinically, patients may remain asymptomatic for long periods. When symptomatic, presentations include headache, seizures, focal neurological deficits, or cognitive changes.
Early identification and appropriate intervention are essential for optimal outcomes.
Case Report
Patient History
A 52-year-old female presented to the neurology outpatient department with complaints of progressive headache and occasional episodes of blurred vision over three months.
The patient reported:
• Persistent dull frontal headache
• Intermittent nausea
• Episodes of visual blurring
• Mild memory disturbances
There was no history of seizures, trauma, or prior neurological illness.
Clinical Examination
On general examination, the patient was conscious and oriented.
Vital signs were within normal limits.
Neurological examination revealed:
• Glasgow Coma Scale (GCS): 15/15
• Mild bilateral papilledema on fundoscopic examination
• No motor or sensory deficits
• Normal cranial nerve function
No signs of systemic illness were observed.
Clinical Evaluation
Differential Diagnosis
Based on clinical findings, the following conditions were considered:
• Intracranial tumor (primary or secondary)
• Meningioma
• Glioma
• Brain metastasis
• Intracranial hypertension
Further imaging was advised for confirmation.
Investigations
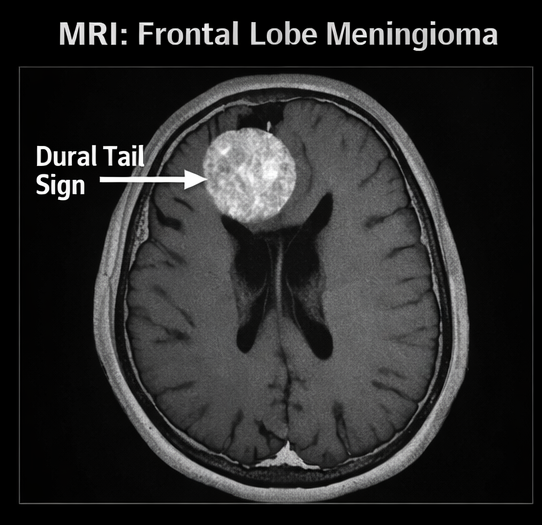
Magnetic Resonance Imaging (MRI) of Brain
MRI with contrast revealed:
• A well-defined extra-axial mass in the left frontal convexity
• Homogeneous contrast enhancement
• Dural tail sign present
• Mild surrounding edema
• Compression of adjacent brain parenchyma without invasion
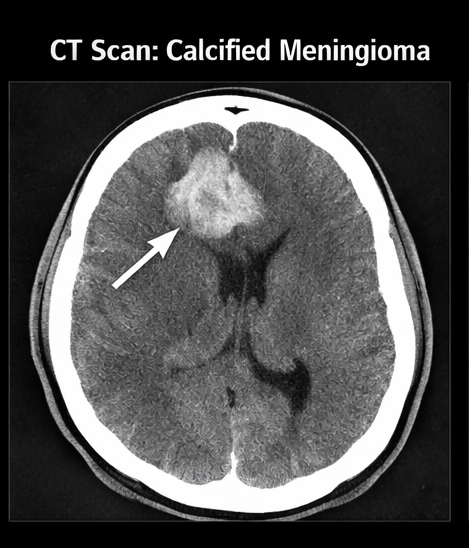
Computed Tomography (CT) Scan
CT scan showed:
• Hyperdense lesion along the frontal convexity
• Evidence of calcification within the tumor
• No hemorrhage
Laboratory Investigations
• Complete blood count: within normal limits
• Renal and liver function tests: normal
• Coagulation profile: normal
Diagnosis
Based on clinical and radiological findings, the diagnosis was:
Left frontal convexity meningioma (likely WHO Grade I)
Management and Outcome
Initial Management
The patient was planned for elective surgical resection.
Preoperative management included:
• Corticosteroids to reduce cerebral edema
• Antiepileptic prophylaxis
• Routine preoperative evaluation
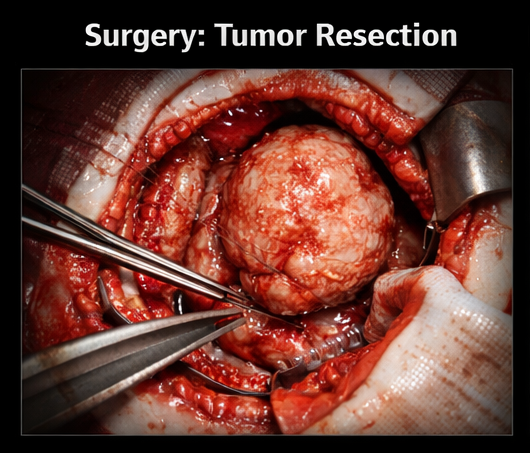
Surgical Intervention
The patient underwent craniotomy with complete excision of the tumor.
Intraoperative findings:
• Well-circumscribed, firm extra-axial tumor
• Clear plane of cleavage from brain tissue
• No significant invasion
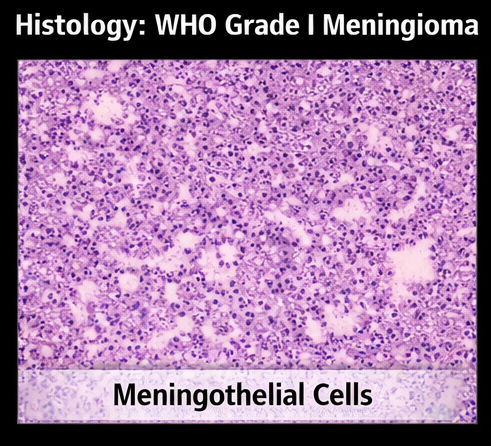
Histopathological Examination
Findings confirmed:
• Meningothelial meningioma (WHO Grade I)
• No atypia or malignancy
Postoperative Course
The patient recovered well post-surgery.
Observations included:
• Resolution of headache
• Improvement in visual symptoms
• No new neurological deficits
Follow-Up
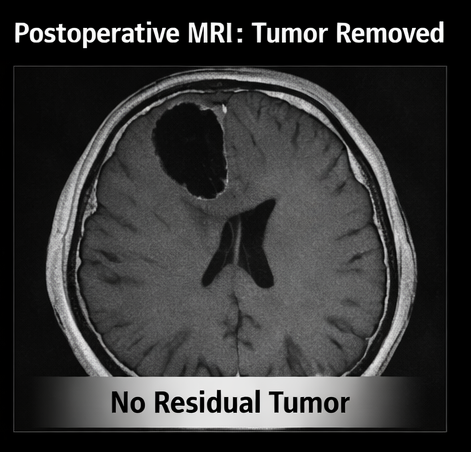
At 3-month follow-up:
• MRI showed no residual tumor
• No recurrence observed
• Patient resumed normal activities
Discussion
Meningiomas are among the most common benign intracranial tumors. Their slow growth often results in delayed clinical presentation, with symptoms primarily due to mass effect.
The frontal lobe is a common site, and tumors in this region may present with subtle cognitive or behavioral changes before neurological deficits become evident.
MRI is the imaging modality of choice due to its superior soft tissue resolution. The presence of a dural tail sign is highly suggestive of meningioma, although not pathognomonic.
Management depends on multiple factors:
• Tumor size and location
• Symptom severity
• Patient age and comorbidities
Treatment options include:
• Observation (for small asymptomatic tumors)
• Surgical resection (gold standard for symptomatic tumors)
• Radiotherapy or stereotactic radiosurgery (for residual or inoperable tumors)
Complete surgical excision (Simpson Grade I resection) is associated with low recurrence rates.
Prognosis is generally excellent for benign meningiomas, with high survival rates and low recurrence when adequately treated.
Conclusion
Meningioma is a common and typically benign intracranial tumor with a favorable prognosis when diagnosed early and managed appropriately. It arises from the meningothelial cells of the arachnoid layer and often demonstrates slow growth, allowing for timely intervention before significant neurological compromise occurs. Most meningiomas are classified as World Health Organization (WHO) Grade I tumors, which are associated with low recurrence rates and excellent long-term survival when treated effectively.
Patients presenting with persistent headaches, progressive neurological symptoms, visual disturbances, or cognitive changes should undergo prompt neuroimaging to rule out intracranial lesions. Early identification is crucial, as delayed diagnosis may lead to complications related to tumor expansion, including mass effect, increased intracranial pressure, and compression of adjacent neural structures.
Magnetic resonance imaging (MRI) plays a pivotal role in diagnosis and surgical planning due to its superior soft tissue resolution and ability to delineate tumor margins, vascular involvement, and surrounding edema. Characteristic imaging features such as homogeneous contrast enhancement and the presence of a dural tail sign can strongly suggest the diagnosis of meningioma, aiding clinicians in differentiating it from other intracranial pathologies.
Surgical resection remains the cornerstone of treatment for symptomatic meningiomas, particularly when the tumor is accessible and causing clinical manifestations. Complete excision not only provides definitive diagnosis through histopathological evaluation but also significantly reduces the risk of recurrence. In selected cases, adjunctive therapies such as radiotherapy or stereotactic radiosurgery may be considered, especially for residual, recurrent, or inoperable tumors. With appropriate management, most patients achieve excellent clinical outcomes, including symptom resolution and a return to normal functional status, as demonstrated in this case.
References
- Louis DN, et al. WHO Classification of Tumors of the Central Nervous System. https://pubmed.ncbi.nlm.nih.gov/30535450/
- Wiemels J, et al. Epidemiology and etiology of meningioma. https://pubmed.ncbi.nlm.nih.gov/24325701/
- Claus EB, et al. Meningioma: review of epidemiology and treatment. https://pubmed.ncbi.nlm.nih.gov/20679936/
- Sughrue ME, et al. Management of meningiomas. https://pubmed.ncbi.nlm.nih.gov/20802304/
- Goldbrunner R, et al. EANO guidelines for the diagnosis and treatment of meningiomas. https://pubmed.ncbi.nlm.nih.gov/31073950/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge