Scabies: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Scabies is a highly contagious parasitic skin infestation caused by Sarcoptes scabiei var. hominis. It commonly presents with intense nocturnal itching, papular eruptions, and characteristic burrows involving the interdigital spaces, wrists, axillae, and genital regions. Delayed diagnosis may lead to secondary bacterial infections, widespread transmission, and significant impairment in quality of life.
We present the case of a 28-year-old male who presented with generalized itching and multiple excoriated papular lesions involving the hands, wrists, abdomen, and groin for 4 weeks. Clinical examination and dermoscopic evaluation confirmed the diagnosis of scabies. The patient was managed with topical permethrin therapy, antihistamines, hygiene measures, and simultaneous treatment of close contacts, resulting in significant clinical improvement.
This case highlights the importance of early recognition, prompt treatment, and preventive strategies in controlling scabies transmission and reducing complications.
Introduction
Scabies is a common ectoparasitic infestation caused by the mite Sarcoptes scabiei. The female mite burrows into the superficial layers of the skin, causing hypersensitivity reactions that result in severe itching and inflammatory skin lesions.
Scabies affects individuals of all age groups and is particularly prevalent in crowded living conditions, institutions, and areas with poor hygiene. Transmission mainly occurs through prolonged skin-to-skin contact, although indirect transmission through contaminated clothing and bedding may also occur.
Important risk factors include:
- Overcrowding
- Poor personal hygiene
- Close household contact
- Immunocompromised state
- Institutional living
- Low socioeconomic conditions
Patients commonly present with:
- Severe nocturnal itching
- Papules and vesicles
- Burrows in interdigital spaces
- Excoriations due to scratching
- Secondary bacterial infection
Delayed diagnosis may lead to persistent infestation, eczema, impetigo, cellulitis, and community outbreaks. Early diagnosis and simultaneous treatment of contacts are essential for disease control.
Case Report
Patient History
A 28-year-old male presented to the dermatology outpatient department with:
- Severe itching for 4 weeks
- Increased itching during night
- Multiple red raised lesions over hands and abdomen
- Sleep disturbance due to pruritus
The patient reported that two family members had similar symptoms.
There was no history of:
- Drug allergy
- Chronic skin disease
- Diabetes mellitus
- Recent travel
Clinical Examination
General Examination
-
Afebrile
-
Pulse rate: 82/min
-
Blood pressure: 118/76 mmHg
-
Systemically stable
Dermatological Examination
Cutaneous examination revealed:
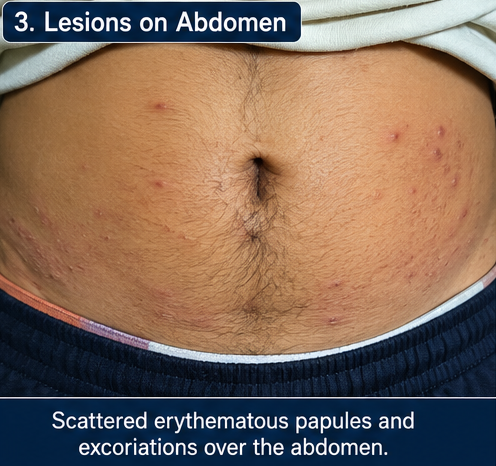
- Multiple erythematous papules
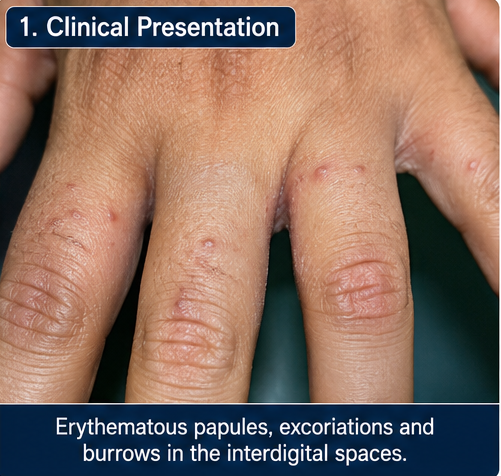
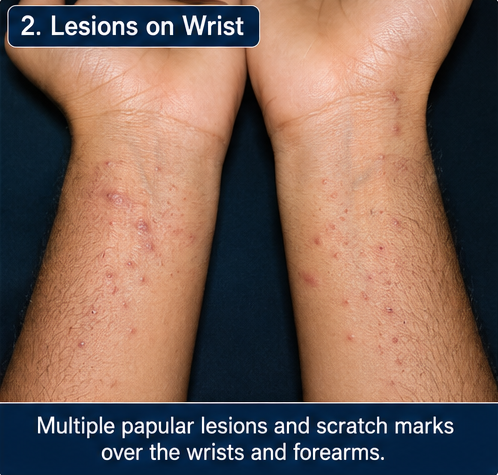
- Excoriated lesions over wrists and abdomen
- Burrows in interdigital spaces
- Papulovesicular lesions in groin region
- Scratch marks with mild crusting
No mucosal involvement was noted.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
- Atopic dermatitis
- Contact dermatitis
- Papular urticaria
- Fungal infection
- Scabies
The presence of nocturnal itching, burrows, and family history strongly suggested scabies infestation.
Investigations
Laboratory Findings
- Complete blood count: Normal
- Blood sugar levels: Normal
- No eosinophilia detected
Dermoscopy
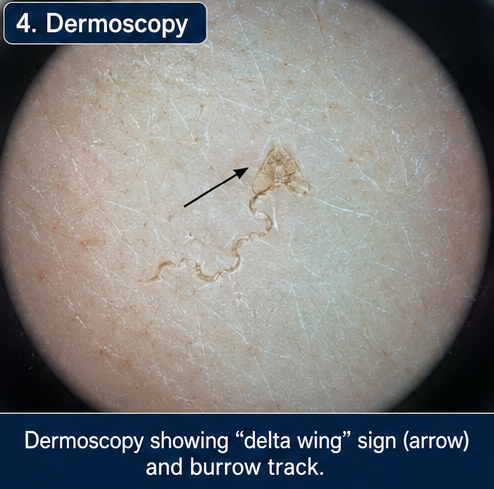
Dermoscopy revealed:
- Characteristic “delta wing” appearance
- Burrow tracks
- Mite visualization
Skin Scraping Examination

Microscopic examination demonstrated:
- Scabies mites
- Eggs
- Fecal pellets (scybala)
These findings confirmed the diagnosis of scabies.
Diagnosis
Based on clinical findings and microscopic examination, a diagnosis of Classical Scabies Infestation was established.
Management and Outcome
Initial Management
The patient was advised:
- Personal hygiene maintenance
- Washing clothes and bedding in hot water
- Avoiding close skin contact
- Simultaneous treatment of family members
Definitive Treatment
The patient received:
-
Topical permethrin 5% cream overnight application
-
Oral antihistamines for itching
-
Mild topical corticosteroid for inflammation
Treatment was repeated after one week.
Follow-Up and Clinical Course
At 2 Weeks
-
Significant reduction in itching
-
Decrease in papular lesions
-
Improved sleep quality
At 4 Weeks
-
Complete resolution of active lesions
-
No fresh burrows
-
Minimal residual pigmentation
At 6 Weeks
-
No recurrence of symptoms
-
Family members also improved after treatment
-
Patient resumed normal daily activities

Discussion
Pathophysiology
Scabies results from infestation by Sarcoptes scabiei mites that burrow into the epidermis and trigger delayed hypersensitivity reactions.
Important pathological mechanisms include:
- Mite burrowing within skin
- Immune-mediated inflammatory response
- Hypersensitivity to mite proteins and feces
- Secondary bacterial colonization due to scratching
Persistent scratching may cause skin barrier disruption and secondary infection.
Epidemiology
Important epidemiological features include:
- Common in tropical and resource-limited regions
- Affects all age groups
- Highly contagious within households
- Increased prevalence in overcrowded settings
- Frequent outbreaks in schools and institutions
Scabies remains an important global public health concern.
Clinical Manifestations
Common symptoms include:
-
Intense nocturnal pruritus
-
Burrows and papules
-
Vesicular lesions
-
Excoriations and crusting
-
Secondary bacterial infection
Commonly involved sites include:
- Finger webs
- Wrists
- Axillae
- Waistline
- Groin
Diagnostic Considerations
Diagnosis is primarily clinical but may be confirmed through:
-
Dermoscopy
-
Skin scraping microscopy
-
Adhesive tape test
-
Histopathology in selected cases
Dermoscopy significantly improves rapid bedside diagnosis.
Treatment Modalities
Medical Management
Conservative measures include:
-
Personal hygiene
-
Contact tracing
-
Environmental decontamination
-
Washing contaminated fabrics
Pharmacological Therapy
Definitive treatment options include:
- Permethrin 5% cream
- Oral ivermectin
- Sulfur ointment
- Benzyl benzoate lotion
- Antihistamines for pruritus
Simultaneous treatment of close contacts is essential to prevent reinfestation.
Complications
Potential complications include:
- Secondary bacterial infection
- Impetigo
- Cellulitis
- Post-scabetic eczema
- Crusted scabies
- Community outbreaks
Untreated scabies may significantly affect quality of life and mental well-being.
Prognosis
Prognosis is excellent with early diagnosis and proper treatment.
Important prognostic factors include:
- Treatment adherence
- Simultaneous contact management
- Personal hygiene
- Prevention of reinfestation
- Early recognition of recurrence
Most patients recover completely with timely therapy.
Conclusion
Scabies is a highly contagious parasitic dermatological disorder caused by infestation with Sarcoptes scabiei var. hominis. The condition remains a significant public health concern, particularly in crowded living conditions, resource-limited settings, schools, nursing homes, and among individuals with close household contact. Transmission primarily occurs through prolonged skin-to-skin contact, although indirect spread through contaminated clothing, towels, bedding, and fomites may also occur. Clinically, patients commonly present with severe nocturnal pruritus, erythematous papules, excoriated lesions, vesicles, nodules, and characteristic serpiginous burrows, most frequently involving the interdigital spaces, flexor aspects of the wrists, axillae, waistline, buttocks, and genital region. Persistent itching and sleep disturbance often lead to considerable physical discomfort, psychological stress, and impaired quality of life. If left untreated, scabies may predispose patients to secondary bacterial infections such as impetigo, cellulitis, and, in severe cases, post-streptococcal complications including glomerulonephritis.
This case emphasizes the importance of maintaining a high index of suspicion in patients presenting with generalized pruritus and typical lesion distribution, especially when there is a history of similar symptoms among close family members or contacts. Accurate diagnosis relies on careful clinical evaluation supported by dermoscopic identification of the classic “delta wing” sign and microscopic confirmation of mites, eggs, or scybala from skin scrapings. Early and appropriate treatment with anti-scabetic agents such as permethrin or ivermectin can rapidly control infestation and prevent further transmission. Equally important is the simultaneous treatment of household members and close contacts, even if asymptomatic, to minimize the risk of reinfestation. Comprehensive patient counseling regarding personal hygiene, environmental cleaning, washing of clothes and bedding in hot water, and adherence to therapy is essential for successful eradication. This case further highlights the role of patient education, follow-up assessment, and preventive public health measures in reducing recurrence, limiting outbreaks, and ensuring complete clinical recovery.
References
- Chosidow O. Scabies and pediculosis. https://pubmed.ncbi.nlm.nih.gov/15459669/
- Engelman D, Cantey PT, Marks M, et al. The public health control of scabies. https://pubmed.ncbi.nlm.nih.gov/31449872/
- Walton SF, Currie BJ. Problems in diagnosing scabies. https://pubmed.ncbi.nlm.nih.gov/15304108/
- Thomas J, Carson CF, Peterson GM, et al. Therapeutic potential of tea tree oil for scabies. https://pubmed.ncbi.nlm.nih.gov/22453108/
- World Health Organization. Scabies Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/scabies
- American Academy of Dermatology. Scabies Overview. AAD Scabies Overview
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge