Umbilical Hernia: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Umbilical hernia is a common pediatric condition characterized by protrusion of intra-abdominal contents through a defect in the umbilical ring due to incomplete closure after birth. It is frequently observed in infants and young children, particularly in those with low birth weight or prematurity. Although most cases are asymptomatic and resolve spontaneously, complications such as incarceration and strangulation may occur, requiring timely surgical intervention. Diagnosis is primarily clinical, supported by imaging in selected cases. Management depends on age, size of the defect, and symptomatology. This case report presents a typical case of umbilical hernia in a young child, highlighting clinical features, diagnostic evaluation, management approach, and favorable outcome following conservative treatment.
Introduction
Umbilical hernia is one of the most common congenital abdominal wall defects encountered in pediatric practice. It results from incomplete closure of the umbilical ring after the detachment of the umbilical cord. The condition is particularly prevalent in neonates and infants, with higher incidence reported in premature infants and those with low birth weight.
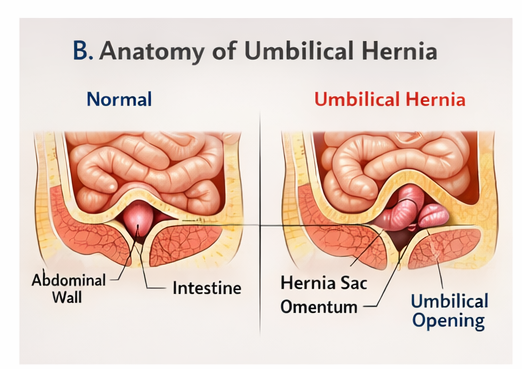
The pathogenesis involves a defect in the fascial ring at the umbilicus, allowing abdominal contents such as omentum or bowel loops to protrude. Increased intra-abdominal pressure from crying, coughing, or straining can accentuate the hernia.
Epidemiologically, umbilical hernias are more common in children of African and Asian descent and show a slight male predominance. Although the exact etiology remains unclear, contributing factors include genetic predisposition, connective tissue weakness, and environmental influences.
Clinically, the condition is usually benign and self-limiting. Most umbilical hernias close spontaneously by the age of 3 to 5 years. However, persistence beyond this age or development of complications necessitates surgical repair.
The clinical course can be divided into stages:
- Early stage: Small, reducible swelling noticeable during increased intra-abdominal pressure
- Intermediate stage: Persistent swelling with gradual enlargement
- Complicated stage: Irreducibility, pain, or signs of bowel obstruction
Risk factors include prematurity, low birth weight, family history, and conditions that increase intra-abdominal pressure.
Early diagnosis and regular follow-up are essential to ensure timely intervention and prevent complications.
Case Report
Patient History
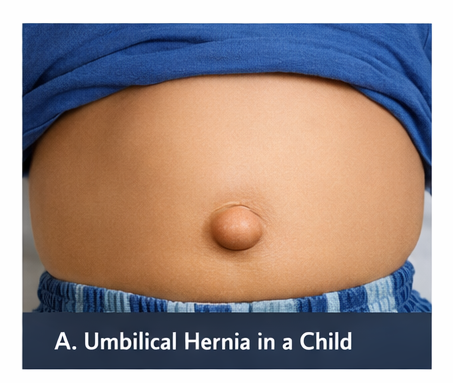
A 2-year-old male child presented to the pediatric outpatient department with a history of swelling at the umbilical region since infancy. The swelling was initially small but became more noticeable over time, especially during episodes of crying, coughing, or straining.
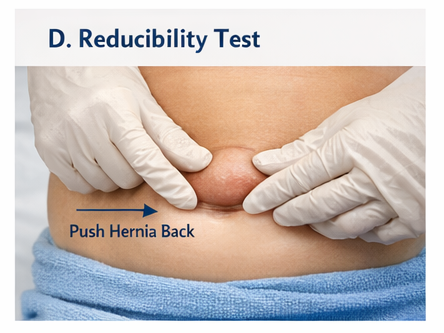
The caregiver reported that the swelling reduced spontaneously when the child was calm or lying down. There was no history of pain, vomiting, abdominal distension, constipation, or any signs of bowel obstruction.
The child had a normal birth history, being delivered at term via normal vaginal delivery. Developmental milestones were appropriate for age, and immunizations were up to date. There was no significant past medical or surgical history.
Clinical Examination
On general examination, the child appeared active, playful, and well-nourished.
Vital signs were stable:
- Temperature: 36.7°C
- Heart rate: 102 beats per minute
- Respiratory rate: 22 breaths per minute
- Blood pressure: within normal limits for age
Local examination of the abdomen revealed:
- A soft, non-tender swelling at the umbilicus measuring approximately 2 cm in diameter
- The swelling increased on crying and decreased on gentle manual pressure
- Presence of an expansile cough impulse
- Overlying skin appeared normal without discoloration or ulceration
No signs of incarceration, strangulation, or inflammation were observed.
Systemic examination, including cardiovascular, respiratory, and neurological systems, was unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on clinical findings, the following differential diagnoses were considered:
- Paraumbilical hernia
- Epigastric hernia
- Umbilical granuloma
- Diastasis recti
- Omphalocele (unlikely due to age and presentation)
The reducibility, location, and characteristic features strongly suggested umbilical hernia.
Investigations
Laboratory Findings
Routine laboratory investigations were within normal limits:
- Complete blood count: normal
- No evidence of infection or inflammation
Imaging
An abdominal ultrasound was performed to confirm the diagnosis and rule out complications:
- Fascial defect at the umbilical ring measuring approximately 1.8 cm
- Herniation of omental fat through the defect
- No bowel loops involved
- No evidence of incarceration or strangulation
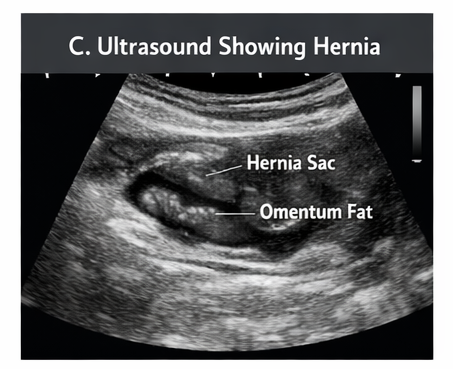
These findings confirmed an uncomplicated umbilical hernia.
Diagnosis
Based on the clinical presentation and imaging findings, the diagnosis was established as:
Uncomplicated Umbilical Hernia
Management and Outcome
Initial Management
Given the child’s age and absence of complications, a conservative approach was adopted. The management plan included:
- Parental reassurance regarding the benign nature of the condition
- Observation with regular follow-up
- Education on warning signs such as pain, irreducibility, vomiting, or discoloration
No immediate surgical intervention was deemed necessary.
Follow-Up Management
The patient was followed at regular intervals of six months. During each visit, the following parameters were assessed:
- Size of the hernia defect
- Reducibility
- Presence of any complications
Parents were advised to avoid applying external pressure devices or traditional remedies.
Outcome
At follow-up visits over the next two years:
- Gradual reduction in the size of the hernia was observed
- The swelling became less prominent over time
- No episodes of incarceration or complications occurred
By the age of 4 years:
- Complete spontaneous closure of the umbilical defect was noted
- The child remained asymptomatic and active
- No surgical intervention was required
Discussion
Umbilical hernia is a frequently encountered condition in pediatric populations, with most cases following a benign course. The condition arises due to failure of complete closure of the umbilical ring, allowing abdominal contents to protrude.
Diagnosis is primarily clinical and based on characteristic findings such as reducible swelling and cough impulse. Imaging is not routinely required but can be useful in atypical cases or when complications are suspected.
The natural history of umbilical hernia is favorable, with spontaneous closure occurring in the majority of cases by 3–5 years of age. Conservative management is therefore the standard approach in asymptomatic children.
Surgical repair is indicated under specific conditions:
- Persistence beyond 5 years of age
- Large defects (greater than 2 cm)
- Complications such as incarceration or strangulation
- Cosmetic concerns or parental preference
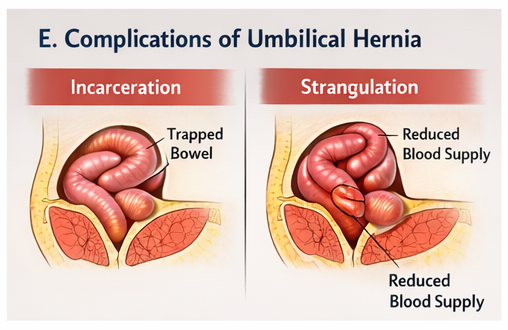
Complications, though rare, can include incarceration, leading to bowel obstruction, and strangulation, which may result in ischemia and necrosis of herniated contents.
Ultrasound plays a supportive role in confirming the diagnosis and evaluating the contents of the hernia sac. It is particularly useful in differentiating umbilical hernia from other abdominal wall defects.
The prognosis is excellent, especially in uncomplicated cases managed conservatively. Surgical outcomes, when required, are also highly favorable with low recurrence rates.
This case reinforces the importance of a conservative approach and highlights the role of regular monitoring in achieving optimal outcomes without unnecessary intervention.
Conclusion
Umbilical hernia is a common and generally benign pediatric condition characterized by a reducible swelling at the umbilicus. It is typically diagnosed clinically and has a high rate of spontaneous resolution.
Conservative management with regular follow-up is appropriate in most cases, particularly in children under five years of age. Early recognition of complications is essential to prevent adverse outcomes.
This case demonstrates that timely diagnosis, appropriate monitoring, and parental education can lead to complete recovery without the need for surgical intervention Awareness among clinicians and caregivers plays a crucial role in ensuring favorable outcomes and avoiding unnecessary procedures.
References
- Zens T, et al. Umbilical Hernias in Children: Outcomes and Management. https://pubmed.ncbi.nlm.nih.gov/26860450/
- Blumberg NA. Infant Umbilical Hernia. https://pubmed.ncbi.nlm.nih.gov/23932620/
- Lassaletta L, et al. The Management of Umbilical Hernias in Children. https://pubmed.ncbi.nlm.nih.gov/15213877/
- Ameh EA, et al. Complications of Umbilical Hernia in Children. https://pubmed.ncbi.nlm.nih.gov/19159752/
- Snyder CL. Current Management of Umbilical Hernias. https://pubmed.ncbi.nlm.nih.gov/24703095/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge