Porokeratosis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Porokeratosis is a rare disorder of keratinization characterized by annular plaques with elevated hyperkeratotic borders and central atrophy. The disease may present in several clinical variants and is considered a premalignant dermatological condition due to its potential for malignant transformation into squamous cell carcinoma or basal cell carcinoma. The condition commonly affects sun-exposed areas and may be associated with genetic predisposition, immunosuppression, chronic sun exposure, and systemic illnesses.
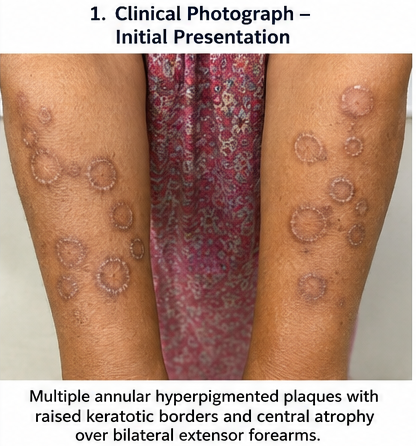
We report the case of a 48-year-old female who presented with slowly progressive hyperpigmented annular plaques over the bilateral forearms and lower legs associated with mild itching and cosmetic concern for nearly three years. Clinical examination and dermoscopic evaluation suggested porokeratosis, which was later confirmed by histopathological examination demonstrating the characteristic cornoid lamella. The patient was managed with topical retinoids, sun protection measures, and cryotherapy for selected lesions, resulting in symptomatic improvement and stabilization of disease progression.
This case highlights the importance of early diagnosis, dermoscopic assessment, histopathological confirmation, regular surveillance for malignant transformation, and individualized therapeutic strategies in the management of porokeratosis.
Introduction
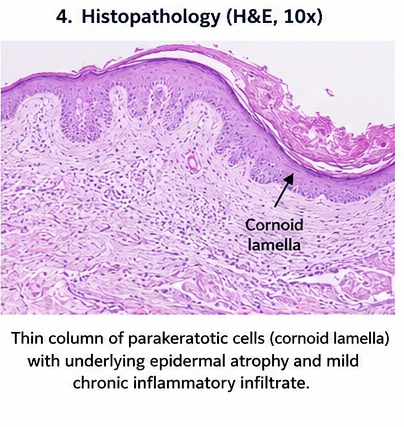
Porokeratosis is a chronic keratinization disorder characterized by abnormal epidermal differentiation resulting in distinct annular lesions with raised keratotic borders. The hallmark histopathological feature is the presence of a cornoid lamella, which represents a thin column of parakeratotic cells extending through the stratum corneum.
The disease was first described by Mibelli in 1893 and includes several clinical variants such as:
- Porokeratosis of Mibelli
- Disseminated superficial actinic porokeratosis (DSAP)
- Linear porokeratosis
- Palmoplantar porokeratosis
- Punctate porokeratosis
- Disseminated superficial porokeratosis
Disseminated superficial actinic porokeratosis is among the most common variants and frequently affects middle-aged adults exposed to chronic ultraviolet radiation.
Important risk factors include:
- Chronic sun exposure
- Genetic predisposition
- Immunosuppression
- Organ transplantation
- HIV infection
- Long-term corticosteroid therapy
- Chronic liver disease
- Autoimmune disorders
- Advancing age
- Fair skin complexion
Clinical manifestations vary according to the subtype and extent of disease involvement.
Common symptoms include:
- Annular hyperpigmented plaques
- Raised keratotic borders
- Mild itching
- Dryness of skin
- Cosmetic disfigurement
- Photosensitivity
- Slowly progressive lesions
Because porokeratosis is considered a premalignant condition, early diagnosis and regular dermatological monitoring are essential to prevent complications.
Case Report
Patient History
A 48-year-old female presented to the dermatology outpatient department with:
- Multiple hyperpigmented skin lesions over both forearms and legs
- Gradual increase in lesion size over 3 years
- Mild itching over affected areas
- Increased lesion prominence after sun exposure
- Cosmetic concern due to visible plaques
The lesions initially appeared as small brownish papules and progressively enlarged over time forming annular plaques with raised margins.
The patient denied:
- Pain
- Bleeding from lesions
- Ulceration
- Fever
- Joint pain
- Weight loss
- Similar lesions in childhood
Past medical history revealed:
- Controlled hypertension
- Chronic outdoor occupational exposure
- No history of immunosuppressive therapy
- No known family history of similar skin disease
Clinical Examination
General Examination
- Conscious and oriented
- Afebrile
- Pulse rate: 80/min
- Blood pressure: 128/82 mmHg
- Hemodynamically stable
Dermatological Examination
Cutaneous examination revealed:
- Multiple annular hyperpigmented plaques
- Raised keratotic ridge-like borders
- Central atrophic areas
- Bilateral symmetrical distribution
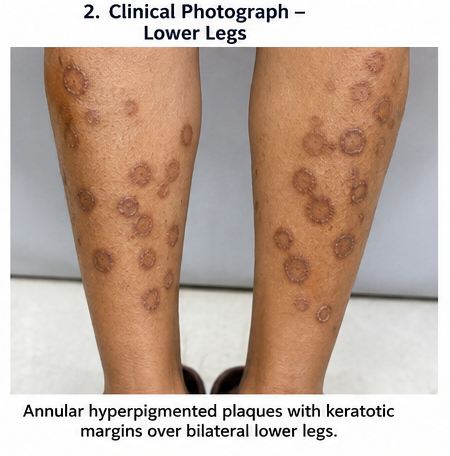
- Lesions predominantly over extensor forearms and lower legs
- Mild scaling at lesion margins
- No active ulceration
- No secondary bacterial infection
The largest lesion measured approximately 4 cm in diameter.
Hair, nails, and mucosal examination were unremarkable.
No regional lymphadenopathy was noted.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
- Porokeratosis
- Tinea corporis
- Discoid lupus erythematosus
- Psoriasis
- Lichen planus
- Actinic keratosis
- Bowen disease
The characteristic keratotic border and annular morphology strongly suggested porokeratosis.
Investigations
Laboratory Findings
Routine laboratory investigations showed:
- Hemoglobin: Normal
- White blood cell count: Normal
- Blood glucose levels: Normal
- Liver function tests: Normal
- Renal function tests: Normal
- HIV serology: Negative
Dermoscopy
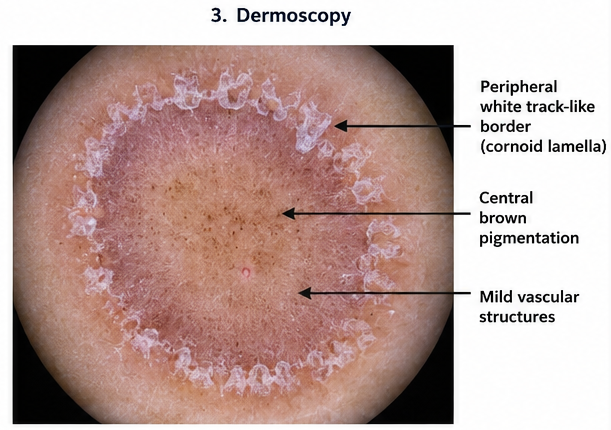
Dermoscopy demonstrated:
- Peripheral white track-like border
- Central brown pigmentation
- Mild vascular changes
- Keratotic rim corresponding to cornoid lamella
Skin Biopsy
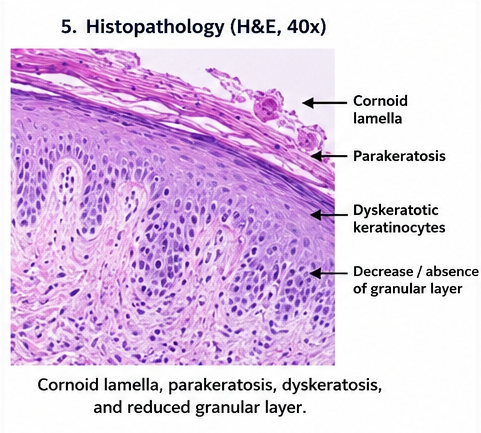
Histopathological examination revealed:
- Presence of cornoid lamella
- Focal parakeratosis
- Dyskeratotic keratinocytes
- Reduced granular layer beneath cornoid lamella
- Mild chronic inflammatory infiltrate
The biopsy findings confirmed the diagnosis of porokeratosis.
Diagnosis
Based on clinical findings, dermoscopic evaluation, and histopathological confirmation, a diagnosis of Disseminated Superficial Actinic Porokeratosis (DSAP) was established.
Management and Outcome
Conservative Management
The patient was advised:
- Strict photoprotection
- Regular sunscreen use
- Avoidance of prolonged sun exposure
- Protective clothing
- Regular dermatological follow-up
Medical Therapy
Topical therapy included:
- Topical tretinoin
- Emollients
- Keratolytic agents
- Mild topical corticosteroids for itching
The patient was also advised oral antioxidant supplementation.
Procedural Management
Cryotherapy was performed for selected symptomatic and cosmetically concerning lesions.
Liquid nitrogen application was done in multiple sessions with appropriate intervals.
Follow-Up and Clinical Course
At 1 Month
- Mild reduction in itching
- Improvement in lesion texture
- Reduced scaling
At 3 Months
- Stabilization of lesion progression
- Cosmetic improvement in treated lesions
- Better patient satisfaction
- No new lesions observed
At 6 Months
- Significant improvement in treated plaques
- No evidence of malignant transformation
- Continued adherence to sun protection measures
- Regular dermatological surveillance advised
The patient remained clinically stable during follow-up.

Discussion
Pathophysiology
Porokeratosis results from abnormal epidermal keratinization caused by clonal proliferation of atypical keratinocytes.
Important pathological mechanisms include:
- Defective keratinocyte maturation
- Abnormal epidermal differentiation
- Ultraviolet radiation-induced damage
- Genetic mutations
- Impaired immune surveillance
- Chronic inflammation
The characteristic cornoid lamella represents abnormal keratinocyte proliferation and defective cornification.
Epidemiology
Important epidemiological features include:
- Common in middle-aged and elderly individuals
- Increased prevalence in sun-exposed populations
- Slight female predominance in DSAP
- Familial inheritance observed in some cases
- Higher risk in immunocompromised individuals
- More common in fair-skinned individuals
The incidence of porokeratosis is increasing due to greater ultraviolet exposure and improved recognition of dermatological disorders.
Clinical Manifestations
Clinical manifestations depend upon the subtype and extent of disease.
Common findings include:
- Annular plaques
- Hyperkeratotic borders
- Central atrophy
- Hyperpigmentation
- Mild pruritus
- Photosensitivity
- Cosmetic disfigurement
Linear porokeratosis may carry a higher risk of malignant transformation.
Diagnostic Consideration
Important diagnostic tools include:
- Clinical dermatological examination
- Dermoscopy
- Histopathological examination
- Skin biopsy
- Digital lesion monitoring
Histopathology demonstrating cornoid lamella remains the gold standard diagnostic feature.
Treatment Modalities
Conservative Therapy
Non-invasive management includes:
- Photoprotection
- Sunscreen application
- Emollients
- Observation for stable lesions
Pharmacological Therapy
Medical treatment options include:
- Topical retinoids
- 5-fluorouracil
- Imiquimod
- Vitamin D analogs
- Topical corticosteroids
- Oral retinoids in extensive disease
Procedural Treatment
Procedures commonly used include:
- Cryotherapy
- Laser therapy
- Photodynamic therapy
- Surgical excision
- Electrocautery
Treatment selection depends upon lesion size, location, symptom severity, cosmetic concern, and risk of malignancy.
Malignant Transformation
Porokeratosis is considered a premalignant condition.
Potential malignancies include:
- Squamous cell carcinoma
- Basal cell carcinoma
- Bowen disease
Risk factors for malignant transformation include:
- Long-standing lesions
- Large plaques
- Chronic sun exposure
- Linear porokeratosis
- Immunosuppression
Regular follow-up and lesion surveillance are essential.
Complications
Potential complications include:
- Chronic cosmetic disfigurement
- Secondary infection
- Persistent itching
- Ulceration
- Malignant transformation
- Psychological distress
- Post-inflammatory pigmentation
Delayed diagnosis may increase the risk of progression and skin malignancy.
Prognosis
The prognosis depends upon:
- Clinical subtype
- Extent of lesions
- Sun exposure
- Early diagnosis
- Compliance with treatment
- Presence of immunosuppression
- Regular follow-up
Most patients achieve symptomatic improvement with appropriate treatment and preventive strategies.
Conclusion
Porokeratosis is an uncommon but clinically important keratinization disorder with significant dermatological and oncological implications. Early recognition of annular keratotic plaques, careful dermoscopic evaluation, and histopathological confirmation are essential for accurate diagnosis.
This case emphasizes the importance of individualized management strategies involving sun protection, topical therapy, procedural interventions, and long-term dermatological surveillance to prevent complications and malignant transformation. Early intervention and regular follow-up remain critical in improving patient outcomes and quality of life.
References
- Sertznig P, von Felbert V, Megahed M. Porokeratosis: present concepts. https://pubmed.ncbi.nlm.nih.gov/20180894/
- Kanitakis J. Porokeratoses: an update of clinical, aetiopathogenic and therapeutic features. https://pubmed.ncbi.nlm.nih.gov/11069502/
- Chernosky ME. Disseminated superficial actinic porokeratosis. https://pubmed.ncbi.nlm.nih.gov/6991663/
- Otsuka F, Someya T, Ishibashi Y. Porokeratosis and malignant skin tumors. https://pubmed.ncbi.nlm.nih.gov/6696729/
- American Osteopathic College of Dermatology. Porokeratosis. https://www.aocd.org/page/Porokeratosis
- National Organization for Rare Disorders. Porokeratosis. https://rarediseases.org/rare-diseases/porokeratosis/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Efficacy and safety of intravenous chemotherapy in children with intraocular retinoblastoma
2.
Certain Oral Bacteria May Be a Risk Factor for Head and Neck Cancer
3.
Quads, Frailty, and the Future: Evolving Frontline Strategies in Multiple Myeloma
4.
Top Cancer Centers; Phase III Win in Prostate Cancer; Screening Recs for Anal Cancer
5.
Traveling to Die: The Latest Form of Medical Tourism
1.
HPV and Immunotherapy in Cancer Survivorship: National Cancer Survivors Day Review
2.
Unlocking the Immune Arsenal: A Revolution in Cancer Treatment
3.
Polycythemia Vera: A Historical Perspective and Contemporary Management
4.
The Benefits and Risks of Transurethral Resection of Bladder Tumor
5.
Colon cancer: Risk factors, warning signs and treatment options
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Experts' Opinion on the Goal of Treatment of Patients with Relapsed Adult B-cell ALL
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Blood Cancer- Further Discussion on Genomic Testing & Advancement in Diagnosis and Treatment
4.
Molecular Contrast: EGFR Axon 19 vs. Exon 21 Mutations - Part VII
5.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge