Coccidioidomycosis (Valley Fever): Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Coccidioidomycosis, also known as Valley Fever, is a fungal infection caused by Coccidioides species, primarily Coccidioides immitis and Coccidioides posadasii. It is endemic to arid and semi-arid regions and is acquired through inhalation of airborne arthroconidia. The clinical spectrum ranges from asymptomatic infection to severe pulmonary and disseminated disease, particularly in immunocompromised individuals. Diagnosis relies on clinical suspicion, serological testing, imaging, and microbiological confirmation. Management varies based on disease severity, ranging from supportive care to antifungal therapy. This case report describes a young adult presenting with pulmonary coccidioidomycosis, highlighting clinical features, diagnostic approach, treatment, and favorable outcome following antifungal therapy.
Introduction
Coccidioidomycosis is a systemic fungal infection caused by dimorphic fungi of the genus Coccidioides. These organisms reside in soil and become airborne when the soil is disturbed. Infection occurs following inhalation of spores, which transform into spherules within the lungs.
The disease is endemic to regions such as the southwestern United States, parts of Mexico, and Central and South America. While many infections are asymptomatic, approximately 40% of affected individuals develop symptomatic disease, commonly presenting as community-acquired pneumonia.
Clinical manifestations vary widely, from mild respiratory illness to chronic pulmonary disease or disseminated infection involving the skin, bones, joints, and central nervous system. Early recognition is essential to prevent complications, particularly in high-risk populations such as immunocompromised patients, pregnant women, and individuals with diabetes.
Case Report
Patient History
A 32-year-old male presented to the outpatient department with complaints of persistent cough, low-grade fever, fatigue, and pleuritic chest pain for three weeks. The patient also reported night sweats and unintentional weight loss of approximately 3 kg over the past month.
He had recently returned from a work assignment in an arid region known for frequent dust exposure. There was no history of tuberculosis contact, smoking, or chronic respiratory illness.
The patient had no significant past medical history and was not on any long-term medications. There was no history of immunosuppression or recent hospitalization.
Clinical Examination
On examination, the patient was mildly febrile (38°C) and appeared fatigued. Vital signs were stable.
Respiratory system examination revealed:
• Mild tachypnea
• Reduced breath sounds over the right lower lung field
• Fine crackles on auscultation
No lymphadenopathy or skin lesions were noted. Cardiovascular and abdominal examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation, the following conditions were considered:
• Community-acquired bacterial pneumonia
• Pulmonary tuberculosis
• Fungal pneumonia (including coccidioidomycosis, histoplasmosis)
• Viral respiratory infection
• Sarcoidosis
The history of travel to an endemic region and dust exposure raised suspicion for coccidioidomycosis.
Investigations
Laboratory Findings
Routine blood investigations revealed:
• Mild leukocytosis
• Eosinophilia (notable finding in some fungal infections)
• Elevated erythrocyte sedimentation rate (ESR)
Chest Imaging
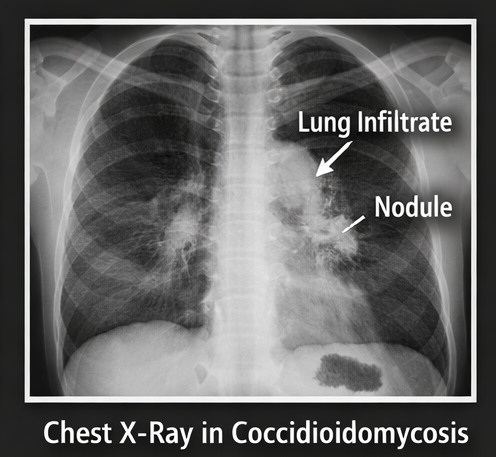
Chest X-ray demonstrated:
• Right lower lobe consolidation
• Ill-defined nodular opacities
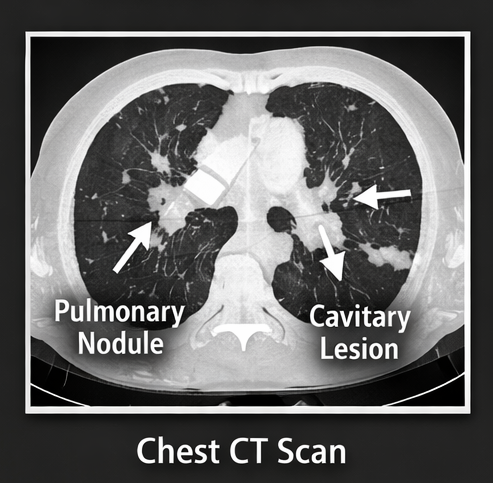
High-resolution CT (HRCT) of the chest revealed:
• Patchy consolidation
• Pulmonary nodules
• Mild hilar lymphadenopathy
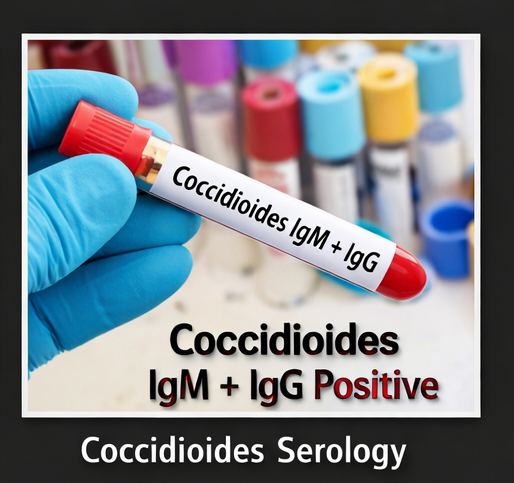
Serological Testing
Coccidioidal serology showed:
• Positive IgM antibodies (suggestive of acute infection)
• Positive IgG antibodies
Microbiological Evaluation
Sputum culture and fungal staining confirmed the presence of Coccidioides species.
Diagnosis
Based on clinical, radiological, serological, and microbiological findings, the diagnosis was established as:
Pulmonary Coccidioidomycosis (Acute Symptomatic Form)
Management and Outcome
Initial Management
The patient was counseled regarding the nature of the disease and treatment options. Given the symptomatic presentation and radiological findings, antifungal therapy was initiated.
Pharmacological Treatment
• Oral fluconazole was started as first-line therapy
• Supportive care including hydration and antipyretics

Follow-Up
At 2 weeks:
• Reduction in fever and cough
• Improved energy levels
At 6 weeks:
• Significant clinical improvement
• Radiological resolution of consolidation
At 3 months:
• Complete symptom resolution
• No progression to chronic or disseminated disease

Outcome
The patient demonstrated:
• Full clinical recovery
• Radiological improvement
• No evidence of complications or dissemination
Discussion
Coccidioidomycosis is an important endemic fungal infection with a wide spectrum of clinical manifestations. The causative organisms exist in soil as mold and convert into spherules in human tissue after inhalation.
The majority of infections are asymptomatic or self-limiting; however, symptomatic patients often present with features resembling community-acquired pneumonia. Common symptoms include cough, fever, chest pain, fatigue, and weight loss.
Risk factors for severe disease include:
• Immunosuppression
• Diabetes mellitus
• Pregnancy
• Advanced age
• Certain ethnic predispositions
Pulmonary involvement is the most common manifestation, but dissemination can occur, particularly to:
• Skin
• Bones and joints
• Central nervous system (meningitis being the most severe form)
Diagnosis is often challenging and requires a combination of:
• Clinical suspicion
• Travel or exposure history
• Imaging findings
• Serological testing (IgM and IgG antibodies)
• Culture or histopathological confirmation
Eosinophilia, although not specific, can be a useful clue in fungal infections such as coccidioidomycosis.
Management depends on disease severity:
• Mild cases may resolve without treatment
• Moderate to severe cases require antifungal therapy
• Fluconazole and itraconazole are commonly used
• Amphotericin B is reserved for severe or disseminated cases
Complications include:
• Chronic pulmonary disease
• Cavitary lung lesions
• Dissemination to extrapulmonary sites
• Coccidioidal meningitis
Preventive strategies include:
• Avoiding dust exposure in endemic areas
• Use of protective masks in high-risk environments
The prognosis is generally favorable in immunocompetent individuals with timely diagnosis and appropriate management.
Conclusion
Coccidioidomycosis is an often underrecognized fungal infection that can mimic common respiratory conditions such as pneumonia or tuberculosis, leading to potential delays in diagnosis. A detailed exposure history, including travel to endemic areas or dust exposure, is essential in raising clinical suspicion. Diagnosis relies on a combination of serological testing for Coccidioides-specific antibodies and imaging findings, which may show pulmonary infiltrates, nodules, or lymphadenopathy.
Most patients, particularly those who are immunocompetent, respond well to antifungal therapy such as fluconazole, with favorable clinical outcomes. However, close follow-up is important to monitor for complications or disease progression. This case highlights the need to consider endemic fungal infections in patients with persistent respiratory symptoms, emphasizing the role of early recognition and appropriate management in improving patient outcomes.
References
- Galgiani JN, Ampel NM, Blair JE, et al. Coccidioidomycosis. https://pubmed.ncbi.nlm.nih.gov/27105387/
- Nguyen C, Barker BM, Hoover S, et al. Recent advances in our understanding of coccidioidomycosis. https://pubmed.ncbi.nlm.nih.gov/31198459/
- Ampel NM. The diagnosis of coccidioidomycosis. https://pubmed.ncbi.nlm.nih.gov/26078093/
- Crum NF, Lederman ER, Stafford CM, et al. Coccidioidomycosis: a descriptive survey. https://pubmed.ncbi.nlm.nih.gov/17599312/
- Saubolle MA, McKellar PP, Sussland D. Epidemiologic, clinical, and diagnostic aspects of coccidioidomycosis. https://pubmed.ncbi.nlm.nih.gov/16156315/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge