Pyogenic Liver Abscess Presenting with Fever, Right Upper Quadrant Pain, and Sepsis in a Middle-Aged Adult: A Case Report
OthersPage Navigation
Abstract
Pyogenic liver abscess (PLA) is a potentially life-threatening intra-abdominal infection characterized by localized pus collection within the hepatic parenchyma. Although uncommon, delayed diagnosis can result in septic shock, rupture, metastatic infection, and multiorgan dysfunction. Predisposing factors include diabetes mellitus, biliary tract disease, abdominal infections, and immunosuppression. Early recognition using laboratory investigations and contrast-enhanced imaging followed by prompt antimicrobial therapy and image-guided drainage significantly improves patient outcomes. We report the case of a 56-year-old man presenting with high-grade fever, right upper quadrant abdominal pain, anorexia, and malaise for one week. Laboratory investigations demonstrated leukocytosis, elevated inflammatory markers, and deranged liver function tests. Contrast-enhanced computed tomography revealed a solitary multiloculated abscess within the right hepatic lobe measuring 7.8 × 6.5 cm. Ultrasound-guided percutaneous catheter drainage combined with broad-spectrum intravenous antibiotics resulted in rapid clinical improvement. The patient recovered completely with resolution of the abscess after six weeks of therapy. This case highlights the importance of early diagnosis, appropriate imaging, microbiological evaluation, and timely drainage in achieving favorable outcomes.
Introduction
Pyogenic liver abscess is the most common visceral abscess and represents a serious bacterial infection of the liver. Improvements in imaging modalities, interventional radiology, and antimicrobial therapy have substantially reduced mortality during recent decades. Nevertheless, delayed diagnosis continues to be associated with significant morbidity and mortality.
The infection commonly develops through ascending biliary tract infection, portal venous spread from intra-abdominal infections, hematogenous dissemination through the hepatic artery, direct extension from adjacent structures, or penetrating trauma. Diabetes mellitus, hepatobiliary malignancy, biliary obstruction, colorectal disease, and immunocompromised states remain important predisposing factors.
Patients frequently present with fever, chills, right upper abdominal pain, nausea, anorexia, weight loss, and generalized weakness. Physical examination may reveal right upper quadrant tenderness, hepatomegaly, and occasionally jaundice. Laboratory abnormalities usually include leukocytosis, elevated C-reactive protein, increased erythrocyte sedimentation rate, elevated alkaline phosphatase, and mild transaminase elevation.
Contrast-enhanced CT remains the diagnostic modality of choice because of its excellent sensitivity in detecting hepatic abscesses and guiding management decisions. Current treatment consists of broad-spectrum antimicrobial therapy combined with image-guided percutaneous drainage for large or complex abscesses.
Case Report
A 56-year-old man presented to the emergency department with high-grade fever associated with chills, right upper abdominal pain, loss of appetite, and generalized weakness for seven days. The abdominal pain was dull, continuous, localized to the right hypochondrium, and aggravated by deep inspiration and movement. He also complained of nausea without vomiting.
His medical history included poorly controlled type 2 diabetes mellitus for ten years and hypertension controlled with medication. There was no previous history of chronic liver disease, viral hepatitis, alcohol dependence, or recent abdominal surgery.
On examination, the patient appeared ill and febrile. His temperature was 39.1°C, pulse rate 108 beats/minute, blood pressure 118/72 mmHg, respiratory rate 22 breaths/minute, and oxygen saturation 97% on room air. Abdominal examination revealed localized tenderness over the right hypochondrium with mild hepatomegaly. There were no signs of generalized peritonitis.
Laboratory investigations demonstrated a total leukocyte count of 18,700 cells/mm³ with neutrophilic predominance, C-reactive protein of 186 mg/L, erythrocyte sedimentation rate of 78 mm/hour, serum bilirubin of 1.8 mg/dL, alkaline phosphatase of 286 IU/L, alanine aminotransferase of 82 IU/L, aspartate aminotransferase of 76 IU/L, serum albumin of 3.1 g/dL, and glycated hemoglobin (HbA1c) of 8.7%. Renal function tests were within normal limits.
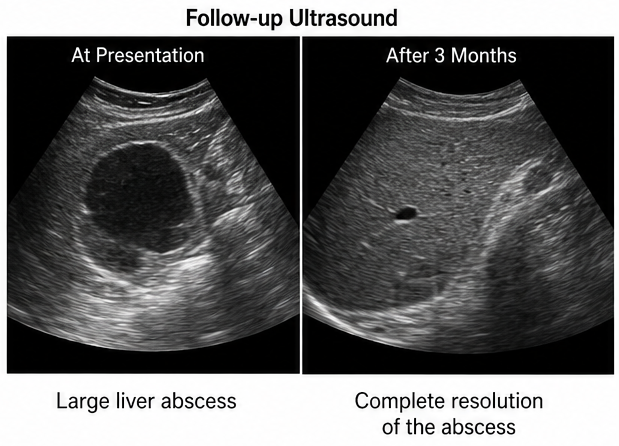
Ultrasonography demonstrated a heterogeneous hypoechoic lesion within the right hepatic lobe.
Contrast-enhanced CT of the abdomen confirmed a multiloculated liver abscess involving segments VII and VIII measuring 7.8 × 6.5 cm with surrounding inflammatory edema.
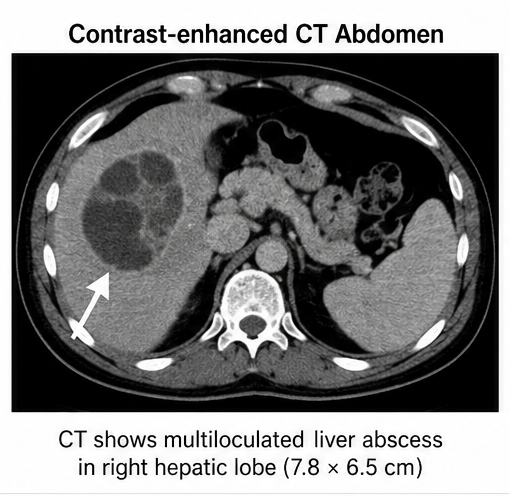
No evidence of rupture or peritoneal collection was identified.
Blood cultures were obtained before initiation of antimicrobial therapy.
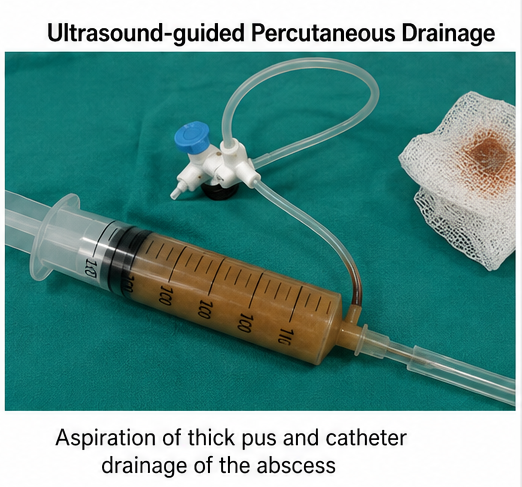
Ultrasound-guided aspiration yielded thick purulent material.
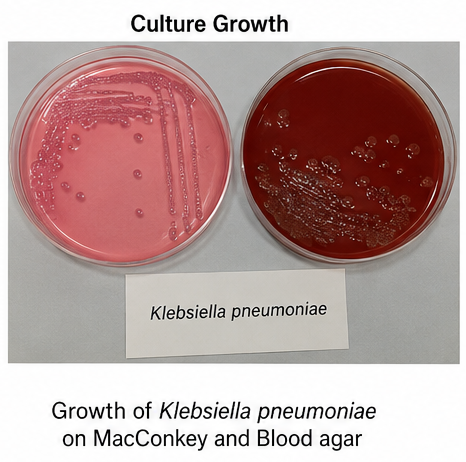
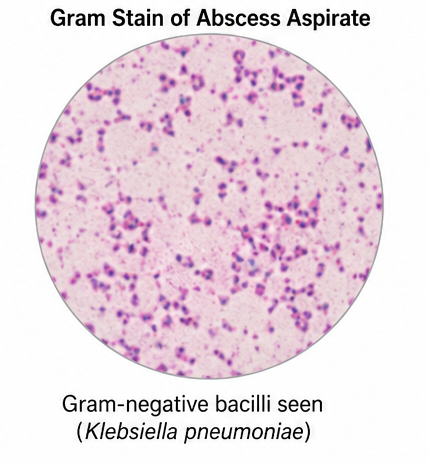
Gram staining revealed Gram-negative bacilli, while culture isolated Klebsiella pneumoniae, sensitive to third-generation cephalosporins and carbapenems.
Based on clinical findings, laboratory investigations, microbiological analysis, and imaging, a diagnosis of pyogenic liver abscess secondary to Klebsiella pneumoniae infection was established.
Management and Outcome
The patient was admitted for intensive monitoring and intravenous antimicrobial therapy. Empirical treatment with intravenous piperacillin-tazobactam and metronidazole was initiated immediately after obtaining blood cultures. Following culture sensitivity results, antimicrobial therapy was streamlined to intravenous ceftriaxone combined with metronidazole.
Because of the large size and multiloculated nature of the abscess, ultrasound-guided percutaneous catheter drainage was performed. Approximately 180 mL of thick purulent material was evacuated, and continuous drainage was maintained for six days until daily output became negligible.
Strict glycemic control was achieved using insulin therapy. Supportive treatment included intravenous fluids, analgesics, nutritional support, and regular monitoring of inflammatory markers and liver function tests.
The patient showed significant clinical improvement within 72 hours, with complete resolution of fever and progressive reduction in abdominal pain. No procedure-related complications occurred.
Follow-up
One Month
- Complete resolution of fever and constitutional symptoms.
- Normal appetite restored.
- Leukocyte count and C-reactive protein returned near normal.
- Ultrasound demonstrated marked reduction in abscess cavity size.
Three Months
- Follow-up CT scan demonstrated complete resolution of the hepatic abscess.
- Liver function tests normalized.
- Percutaneous drainage site healed completely.
- Glycemic control improved with HbA1c reduced to 7.1%.
Six Months
The patient remained asymptomatic with no recurrence of fever or abdominal pain. Repeat ultrasonography showed complete resolution of the abscess without residual cavity. He continued regular follow-up for diabetes management and remained free from recurrent hepatobiliary infection.
Discussion
Pyogenic liver abscess remains an important cause of intra-abdominal sepsis despite advances in diagnostic imaging and antimicrobial therapy. The incidence has increased due to aging populations, diabetes mellitus, hepatobiliary interventions, and improved detection by cross-sectional imaging.
Klebsiella pneumoniae has emerged as the predominant pathogen in many Asian countries and is increasingly recognized worldwide. Unlike polymicrobial biliary infections, Klebsiella liver abscesses may occur in patients without underlying hepatobiliary disease and have a greater propensity for metastatic complications such as endophthalmitis and central nervous system infection.
Contrast-enhanced CT is considered the gold standard imaging modality owing to its high sensitivity and ability to define abscess size, location, multiplicity, and suitability for percutaneous drainage. Blood cultures and abscess cultures remain essential for identifying causative organisms and facilitating targeted antimicrobial therapy.
Current management combines broad-spectrum antibiotics with image-guided drainage for abscesses larger than 3–5 cm, multiloculated collections, or patients with persistent sepsis. Percutaneous catheter drainage has largely replaced surgical drainage because it is minimally invasive, highly effective, and associated with shorter hospital stay and lower morbidity.
Early diagnosis, adequate source control, optimization of underlying comorbidities, and appropriate antimicrobial stewardship remain the cornerstones of successful management.
Prognosis
The prognosis of pyogenic liver abscess has improved substantially with advances in imaging, interventional radiology, and antimicrobial therapy. Most patients recover completely when prompt diagnosis is followed by appropriate drainage and culture-directed antibiotic treatment. However, delayed intervention, uncontrolled diabetes mellitus, multiple abscesses, septic shock, or metastatic infection are associated with poorer outcomes. Long-term follow-up is recommended to ensure complete radiological resolution and prevent recurrence.
Conclusion
Pyogenic liver abscess is a potentially fatal but highly treatable condition when recognized early. Fever, right upper quadrant pain, and elevated inflammatory markers should prompt timely abdominal imaging in high-risk individuals. Contrast-enhanced CT, microbiological confirmation, image-guided drainage, and culture-directed antimicrobial therapy form the cornerstone of management. Comprehensive treatment, control of underlying risk factors, and regular follow-up significantly reduce morbidity, prevent recurrence, and improve long-term clinical outcomes.
References
- Mavilia MG, Molina M, Wu GY. Pyogenic liver abscess: A review of etiology, diagnosis, and management. World Journal of Gastroenterology. 2016;22(3):944–952. https://pubmed.ncbi.nlm.nih.gov/26811646/
- Longworth S, Han J. Pyogenic liver abscess. Clinical Liver Disease. 2015;6(2):51–54. https://pubmed.ncbi.nlm.nih.gov/31040961/
- Kaplan GG, Gregson DB, Laupland KB. Population-based study of the epidemiology of pyogenic liver abscess. Clinical Gastroenterology and Hepatology. 2004;2(11):1032–1038. https://pubmed.ncbi.nlm.nih.gov/15551257/
- Serraino C, Elia C, Bracco C, et al. Characteristics and management of pyogenic liver abscess: A European experience. Medicine (Baltimore). 2018;97(19):e0628. https://pubmed.ncbi.nlm.nih.gov/29768372/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
I Was Told I Had 6 Months to Live. That Was 20 Years Ago.
2.
Which Salvage Therapy Is Best for Recurrent Prostate Cancer?
3.
Aspirin Fails to Boost Survival in Colorectal Cancer Trial
4.
Chemoimmunotherapy Boosts Head and Neck Cancer Response
5.
Researchers use AI to monitor side effects of chemotherapy and support families dealing with pediatric cancer.
1.
Essential Developments in Oncology for Healthcare Excellence
2.
Beta-2 Microglobulin: Function, Role in Disease & Clinical Significance Explained
3.
Understanding Apoplexy: Symptoms, Causes, and Treatment Options
4.
Deciphering FFR: A Comprehensive Guide to Understanding Its Meaning
5.
Understanding the Rare Disease: Werner Syndrome Explained
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Should We Use DARA Up Front As First-Line Therapy in MM?
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Current Scenario of Cancer- Palliative Care to Close the Care Gap
4.
What Therapy Would Yield the Best Outcomes In Patients with R/R B-cell ALL?
5.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC: A Continuation

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge