Diabetic Foot Ulcer: Diagnostic Evaluation, Multidisciplinary Management, and Clinical Outcome — A Case Report
OthersPage Navigation
Abstract
Diabetic foot disease is a serious and common complication of long-standing diabetes mellitus, representing a major cause of morbidity, hospital admissions, and lower-limb amputations worldwide. It arises from a complex interplay of peripheral neuropathy, peripheral arterial disease, infection, and impaired wound healing. Early diagnosis and coordinated multidisciplinary management are critical to limb salvage and patient survival. We report a case of an infected diabetic foot ulcer in a middle-aged man with poorly controlled type 2 diabetes mellitus. Comprehensive clinical assessment, microbiological evaluation, vascular imaging, and metabolic optimization guided a multimodal treatment strategy involving wound care, targeted antibiotic therapy, glycemic control, and surgical intervention. The patient achieved satisfactory wound healing with limb preservation. This case highlights the importance of early recognition, structured assessment, and team-based care in optimizing outcomes in diabetic foot disease.
Introduction
Diabetic foot complications are among the most debilitating sequelae of diabetes mellitus, affecting approximately 15–25% of patients during their lifetime and accounting for up to 85% of diabetes-related amputations [1]. Peripheral neuropathy leads to loss of protective sensation, while peripheral arterial disease compromises tissue perfusion, predisposing patients to ulceration and infection. Once established, diabetic foot ulcers (DFUs) are challenging to treat and are associated with high rates of recurrence, amputation, and mortality [2].
The management of diabetic foot disease requires early diagnosis, accurate assessment of infection and ischemia, and prompt initiation of evidence-based therapy. International guidelines emphasize the role of multidisciplinary foot care teams in reducing complications and improving limb salvage rates [3]. This case report describes the clinical presentation, diagnostic workup, and integrated management of an infected diabetic foot ulcer, illustrating key principles of contemporary care.
Case Report
Patient History
A 56-year-old man presented to the surgical outpatient department with a non-healing ulcer over the plantar aspect of his right foot for six weeks. He reported progressive swelling, foul-smelling discharge, and increasing pain over the past ten days.

The patient had a 12-year history of type 2 diabetes mellitus, with irregular follow-up and suboptimal glycemic control. He also had a history of hypertension but no known coronary artery disease. There was no history of trauma, fever, or prior foot ulcers. The patient admitted to walking barefoot indoors and had not received prior diabetic foot education.
Clinical Examination
On general examination, the patient was afebrile and hemodynamically stable. Pallor was absent, and systemic examination was unremarkable. Local examination of the right foot revealed a 3 × 3 cm ulcer over the plantar surface at the head of the first metatarsal. The ulcer had irregular margins, a necrotic base, and purulent discharge with surrounding erythema and induration.

Peripheral sensory examination revealed loss of vibration and pressure sensation using a 10-g monofilament, consistent with diabetic peripheral neuropathy. Dorsalis pedis and posterior tibial pulses were palpable but reduced in volume. No clinical features of acute limb ischemia were noted.
Investigations
Laboratory Evaluation
Baseline investigations showed poor glycemic control, with a fasting blood glucose of 216 mg/dL and HbA1c of 9.4%. White blood cell count was mildly elevated at 12,500/mm³, and C-reactive protein was raised. Renal and liver function tests were within acceptable limits.
Microbiological Assessment
Deep wound swab culture obtained under aseptic conditions revealed polymicrobial infection, with growth of methicillin-sensitive Staphylococcus aureus and Escherichia coli. Antimicrobial susceptibility testing demonstrated that both organisms were sensitive to beta-lactam antibiotics, including penicillins and cephalosporins, with no evidence of multidrug resistance. These findings supported the diagnosis of a moderate soft tissue infection and enabled targeted antibiotic therapy, facilitating effective infection control and contributing to favorable wound healing.
Radiological and Vascular Assessment
Plain radiography of the foot showed soft tissue swelling without evidence of osteomyelitis.

Duplex Doppler ultrasound of the lower limbs demonstrated mild peripheral arterial disease with preserved distal flow. There was no critical limb ischemia.
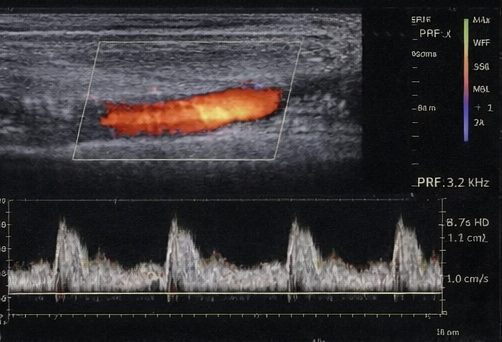
Based on clinical and investigational findings, the condition was classified as a moderate infected diabetic foot ulcer (Wagner grade 2).
Diagnosis
Based on the clinical presentation, neurological findings, microbiological results, and vascular assessment, a diagnosis of an infected diabetic foot ulcer secondary to diabetic peripheral neuropathy was established, with associated mild peripheral arterial disease contributing to impaired wound healing. The absence of critical limb ischemia and radiological evidence of osteomyelitis supported classification as a moderate soft tissue infection, guiding appropriate conservative and surgical management strategies.
Management and Outcome
Multidisciplinary Approach
The patient was managed by a multidisciplinary diabetic foot care team comprising a surgeon, endocrinologist, infectious disease specialist, podiatrist, and wound care nurse.
Treatment
Initial management included hospital admission, strict glycemic control with insulin therapy, and empirical intravenous antibiotics, later tailored according to culture sensitivity. Surgical debridement was performed to remove necrotic tissue and reduce bacterial load.
Regular wound dressings with saline and antimicrobial agents were instituted, along with pressure offloading using customized footwear. The patient received intensive education on foot hygiene, daily inspection, and appropriate footwear use.
Follow-Up
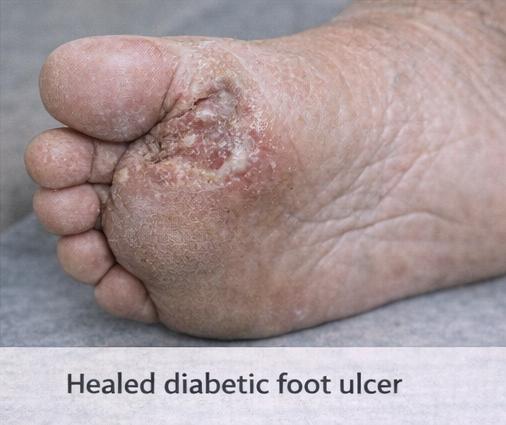
Over four weeks, the ulcer demonstrated progressive granulation and reduction in size. Antibiotics were transitioned to oral therapy, and the patient was discharged with close outpatient follow-up. At three-month review, the ulcer had completely healed, and the patient remained ambulatory with no recurrence. Glycemic control improved, with HbA1c reduced to 7.6%.
Discussion
Diabetic foot ulcers are a leading cause of non-traumatic lower-limb amputations and reflect systemic disease severity rather than a localized problem alone. Peripheral neuropathy plays a central role by allowing repetitive unrecognized trauma, while infection accelerates tissue destruction and systemic complications [4].
This case underscores the importance of early identification of infection severity, assessment of vascular status, and prompt initiation of multidisciplinary care. Surgical debridement combined with appropriate antibiotics and metabolic optimization remains the cornerstone of treatment for infected DFUs [5].
Preventive strategies, including patient education, regular foot examinations, and early referral to specialized foot clinics, are critical in reducing disease burden. Long-term outcomes depend not only on wound healing but also on sustained glycemic control and lifestyle modification.
Conclusion
Diabetic foot disease remains a significant clinical challenge with substantial implications for patient quality of life and healthcare systems. This case highlights that timely diagnosis, structured evaluation, and coordinated multidisciplinary management can achieve limb salvage and favorable clinical outcomes. Prevention through patient education, routine screening, and optimal diabetes control remains the most effective strategy to reduce the incidence and recurrence of diabetic foot complications.
References
- International Diabetes Federation. IDF Diabetes Atlas. 10th ed. Brussels: IDF; 2021.
- Armstrong DG, Boulton AJM, Bus SA. Diabetic foot ulcers and their recurrence. N Engl J Med. 2017;376(24):2367–2375.
- Lipsky BA, et al. IWGDF guidelines on the diagnosis and treatment of foot infection in persons with diabetes. Diabetes Metab Res Rev. 2020;36(S1):e3280.
- Boulton AJM. The diabetic foot: From art to science. Diabetologia. 2004;47(8):1343–1353.
- Lavery LA, et al. Effectiveness and safety of early surgical intervention in diabetic foot infections. Diabetes Care. 2006;29(6):1288–1293.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Does pollution cause cancer?
2.
AI is equally capable of reading breast cancer scans as human radiologists.
3.
EVP Beats Cisplatin for Resectable MIBC
4.
New research points out a promising strategy for treating metastatic medulloblastoma
5.
Academics + Pharma = Big Bucks; New CAR-T Warnings; Patients Seek Cancer Tests.
1.
A Closer Look at Breast Cancer: Examining the Ultrasound Images
2.
Unlocking the Secrets of Oral Cancer Staging: A New Approach to Early Detection
3.
Impact of Hormone Therapy Cessation on Tumor Growth: Case Study of Ki-67 Reduction
4.
Unraveling the Mysteries of Lymphoma: A Journey into the Unknown
5.
Refining AML Survival: Prognostic Factors, Therapies, and Stem Cell Strategies Reviewed
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Navigating the Complexities of Ph Negative ALL - Part III
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Management of 1st line ALK+ mNSCLC (CROWN TRIAL Update)
4.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part III
5.
Virtual Case Study on Pedal Edema and Triple Vessel Disease - An Initiative by Hidoc Dr.

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge