Retinal Hemorrhage: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Retinal hemorrhage is a clinically significant ophthalmic finding characterized by bleeding within the retinal layers due to vascular disruption. It may result from systemic conditions such as hypertension, diabetes mellitus, or localized retinal vascular disorders. Depending on its location and severity, retinal hemorrhage can lead to varying degrees of visual impairment, ranging from mild blurring to sudden vision loss.
We present the case of a 52-year-old male who developed sudden painless diminution of vision in the right eye. Clinical examination and fundoscopic findings revealed multiple flame-shaped retinal hemorrhages associated with hypertensive retinopathy. Prompt systemic and ophthalmologic management led to stabilization of vision and gradual resolution of hemorrhages over time.
This case emphasizes the importance of early diagnosis, comprehensive systemic evaluation, and timely management in preventing permanent visual damage in patients with retinal hemorrhage.
Introduction
Retinal hemorrhages occur when retinal blood vessels rupture or leak, leading to accumulation of blood within different retinal layers. They are broadly classified based on their anatomical location into preretinal, intraretinal, and subretinal hemorrhages. Morphologically, they may present as flame-shaped hemorrhages in the nerve fiber layer or dot-blot hemorrhages in deeper retinal layers.
The etiology of retinal hemorrhage is diverse and includes systemic vascular disorders such as hypertension and diabetes mellitus, retinal vein occlusion, trauma, blood dyscrasias, and coagulopathies. In many cases, retinal hemorrhages serve as an early indicator of systemic disease, making their recognition critical in clinical practice.
Advancements in diagnostic modalities, including fundus photography, optical coherence tomography (OCT), and fluorescein angiography, have enhanced the ability to detect and monitor retinal hemorrhages with precision. Management strategies are directed toward treating the underlying cause and preventing complications such as macular edema or neovascularization.
Case Report
Patient History
A 52-year-old male presented to the ophthalmology clinic with complaints of sudden, painless blurring of vision in the right eye for the past three days. The visual disturbance was not associated with redness, discharge, or photophobia.
The patient reported a history of intermittent headaches over the past six months but had not sought medical attention. He had a known history of hypertension for eight years but admitted to poor compliance with antihypertensive therapy.
There was no history of trauma, diabetes mellitus, bleeding disorders, or use of anticoagulant medications. Family history was unremarkable for ocular or systemic vascular diseases.
Clinical Examination
General Examination
The patient was conscious, alert, and oriented. Vital signs revealed significantly elevated blood pressure at 180/110 mmHg. No signs of anemia, cyanosis, or peripheral edema were observed.
Ophthalmic Examination
Visual acuity testing showed 6/24 vision in the right eye and 6/6 in the left eye. The anterior segment examination was unremarkable in both eyes.
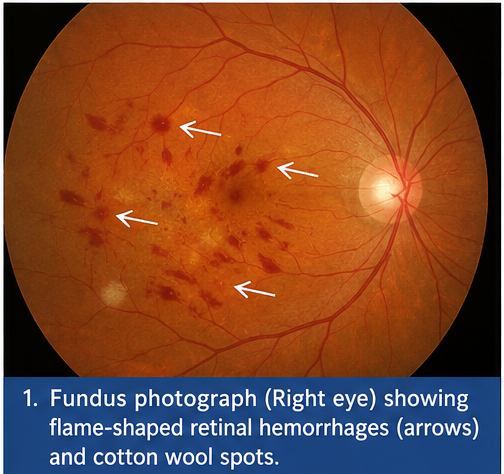
Fundoscopic examination of the right eye revealed multiple flame-shaped hemorrhages along the retinal nerve fiber layer, accompanied by cotton wool spots and generalized arteriolar narrowing. Mild optic disc edema was also noted. The left eye demonstrated early vascular changes, including arteriolar attenuation, but no hemorrhages.
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation and examination findings, the following differential diagnoses were considered:
• Hypertensive retinopathy (most likely)
• Diabetic retinopathy
• Retinal vein occlusion
• Blood dyscrasia-related retinal hemorrhage
• Traumatic retinal hemorrhage
The absence of diabetes, trauma, and systemic hematological abnormalities, along with markedly elevated blood pressure, strongly supported hypertensive retinopathy as the underlying cause.
Investigations
Ophthalmic Imaging
Fundus Photography:
Revealed multiple flame-shaped hemorrhages radiating along the nerve fiber layer, along with cotton wool spots indicating localized retinal ischemia.
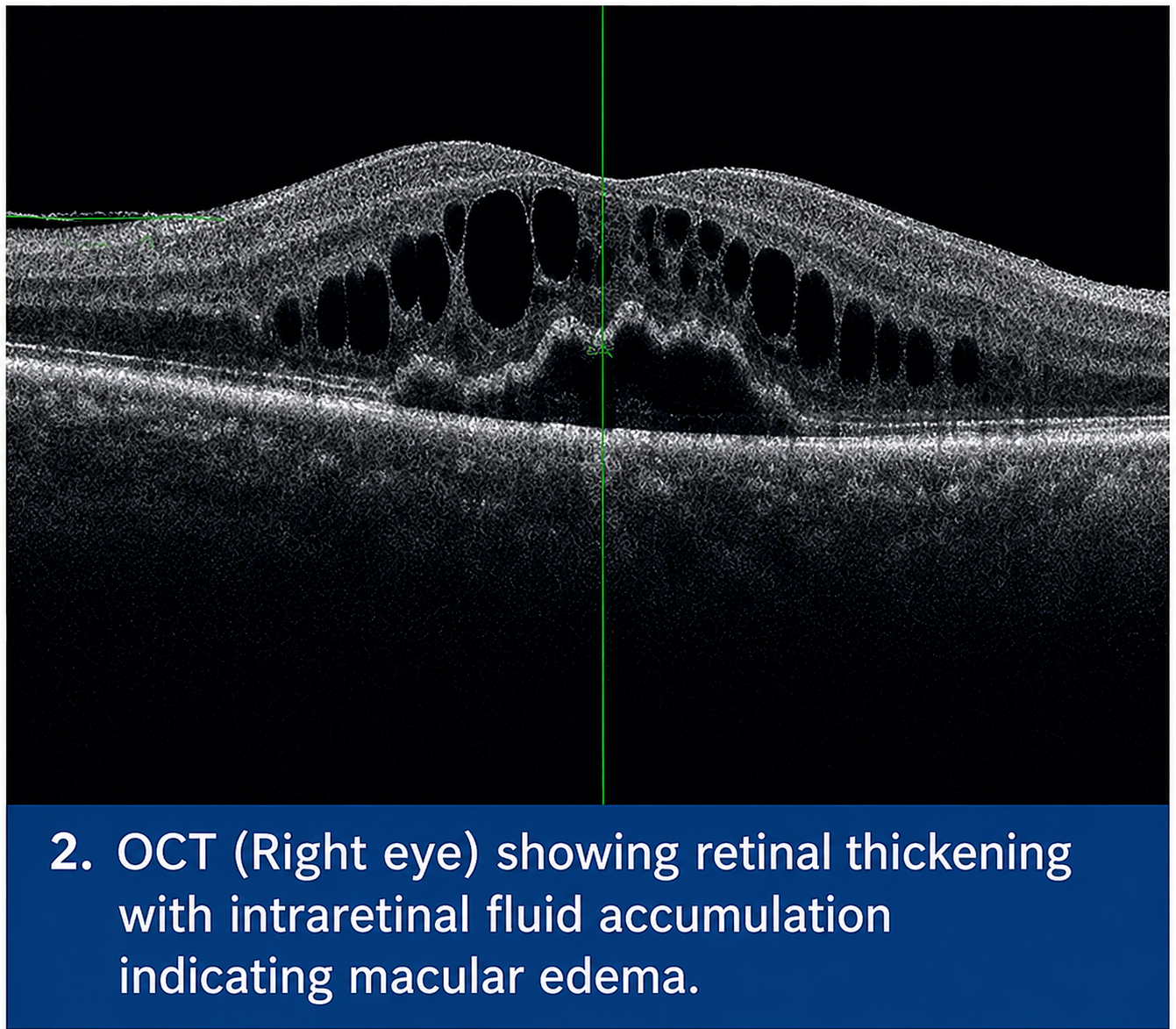
Optical Coherence Tomography (OCT):
Demonstrated retinal thickening with areas of intraretinal fluid accumulation, suggesting vascular leakage.
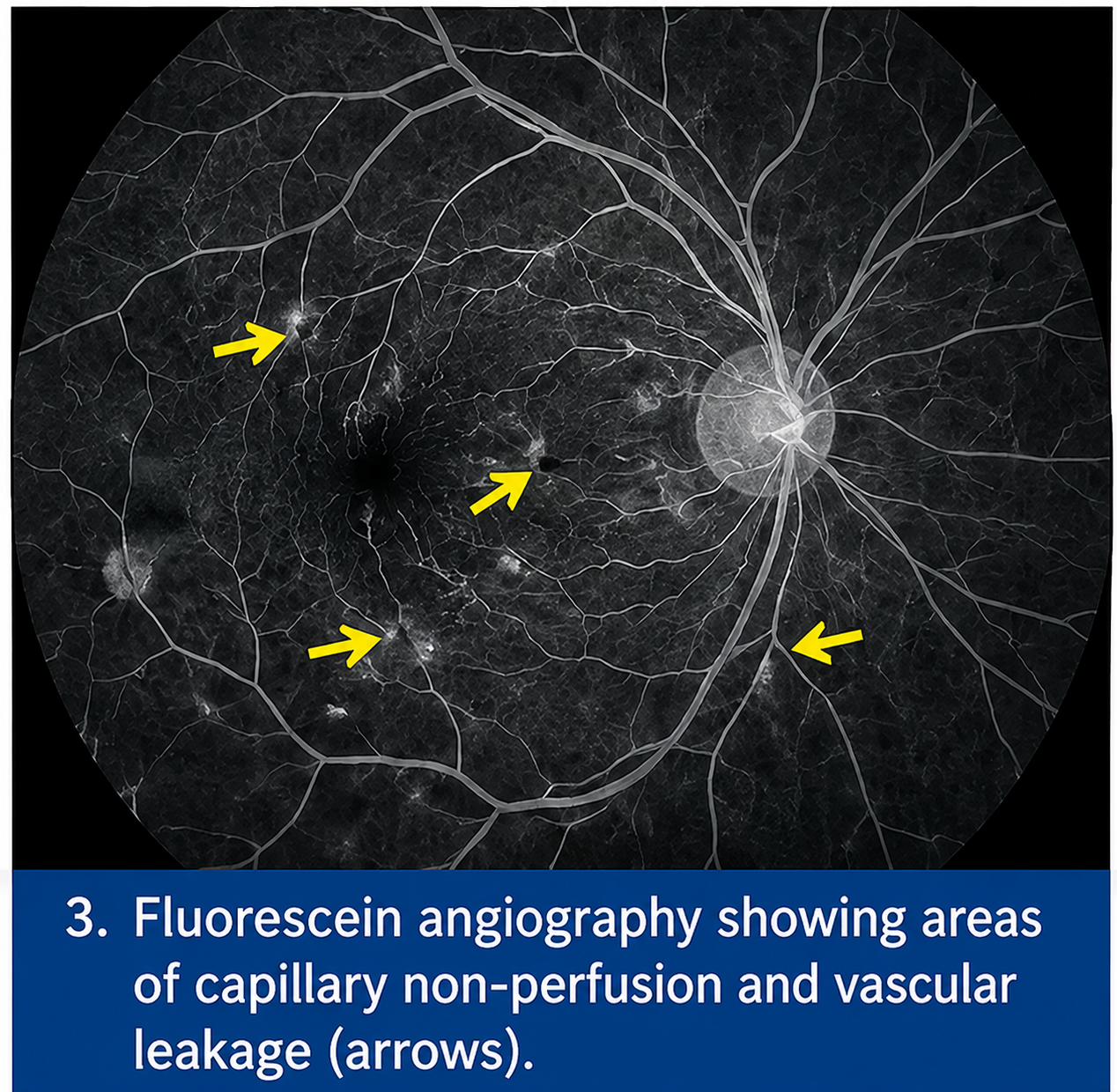
Fluorescein Angiography:
Showed delayed arterial filling, areas of capillary non-perfusion, and leakage from compromised retinal vessels.
Laboratory Investigations
Routine laboratory investigations were performed to assess systemic status:
• Complete blood count: Within normal limits
• Fasting blood glucose: Normal
• Lipid profile: Elevated low-density lipoprotein (LDL) cholesterol
• Renal function tests: Mild elevation in serum creatinine
These findings indicated underlying systemic vascular compromise associated with poorly controlled hypertension.
Diagnosis
A provisional diagnosis of retinal hemorrhage secondary to hypertensive retinopathy was established based on clinical and imaging findings. The presence of characteristic flame-shaped hemorrhages, cotton wool spots, and vascular narrowing strongly indicated chronic hypertensive vascular damage.
The absence of diabetic microvascular changes, such as microaneurysms or neovascularization, and lack of venous tortuosity helped exclude other causes such as diabetic retinopathy and retinal vein occlusion.
Management and Outcome
Management Strategy
The management approach focused on:
• Aggressive control of systemic hypertension
• Prevention of further retinal vascular damage
• Monitoring for potential complications
Medical Management
The patient was initiated on a strict antihypertensive regimen, including combination therapy for optimal blood pressure control. Lifestyle modifications such as dietary sodium restriction, weight management, and regular physical activity were advised.
Lipid-lowering therapy was also initiated to address dyslipidemia and reduce cardiovascular risk.
Ophthalmic Management
The retinal hemorrhages were managed conservatively with close observation. Anti-vascular endothelial growth factor (anti-VEGF) therapy was considered but deferred due to the absence of significant macular edema.
The patient was counseled regarding the importance of strict systemic control and regular ophthalmic follow-up.
Post-Treatment Course
Over the following weeks, the patient showed gradual improvement in visual acuity and reduction in retinal hemorrhages. Blood pressure levels were successfully controlled with medication adherence.
Follow-Up
At 1 Month
Visual acuity improved to 6/12 in the right eye. Fundoscopic examination showed partial resolution of hemorrhages and reduction in cotton wool spots.
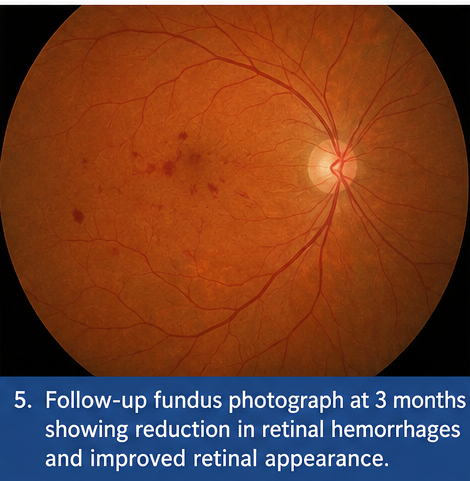
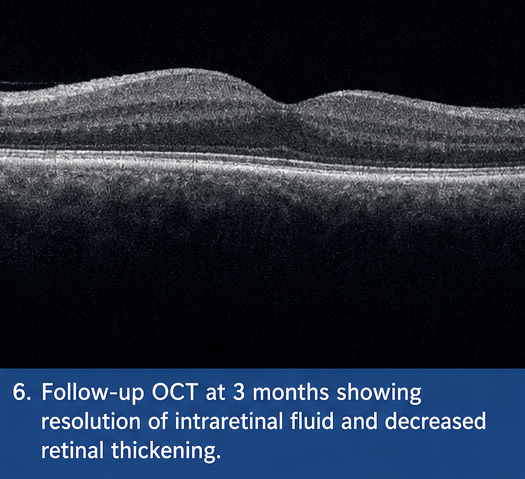
At 3 Months
Significant resolution of retinal hemorrhages was observed. No new lesions were detected, and retinal architecture appeared more stable.
At 6 Months
The patient maintained stable vision with no recurrence of hemorrhages. Blood pressure remained well controlled, and overall functional recovery was excellent.
Discussion
Pathophysiology
Retinal hemorrhages in hypertensive retinopathy occur due to sustained elevation of blood pressure, leading to endothelial damage, increased vascular permeability, and eventual rupture of small retinal vessels. Ischemic injury results in cotton wool spots, while leakage leads to hemorrhage formation.
Etiology and Risk Factors
Common causes of retinal hemorrhage include:
• Systemic hypertension
• Diabetes mellitus
• Retinal vein occlusion
• Trauma
• Hematological disorders
• Anticoagulant therapy
Chronic hypertension remains one of the leading causes, particularly in middle-aged and elderly individuals.
Epidemiology
Retinal hemorrhages are frequently encountered in patients with systemic vascular diseases. Hypertensive retinopathy is more common in individuals with long-standing uncontrolled hypertension and contributes significantly to visual morbidity worldwide.
Clinical Manifestations
The clinical presentation varies depending on severity:
• Sudden painless vision loss
• Blurred vision
• Scotomas or visual field defects
• Asymptomatic in early stages
In this case, the patient presented with typical symptoms of blurred vision associated with hypertensive retinal changes.
Diagnostic Considerations
Diagnosis is primarily clinical, supported by imaging:
- Fundoscopic examination remains the cornerstone
- OCT provides detailed structural assessment
- Fluorescein angiography evaluates vascular integrity
Characteristic findings such as flame-shaped hemorrhages and cotton wool spots aid in diagnosis.
Treatment Considerations
Systemic Management
Effective control of underlying systemic conditions, particularly hypertension, is essential to prevent progression.
Ophthalmic Interventions
In severe cases, treatment options may include:
• Anti-VEGF injections for macular edema
• Laser photocoagulation
• Vitrectomy in cases of non-resolving hemorrhage
Emerging Therapies
Recent advances include:
• Novel anti-VEGF agents with longer duration
• AI-based retinal screening tools
• Regenerative therapies targeting retinal repair
Complications
If untreated, retinal hemorrhages can lead to:
• Permanent vision loss
• Macular edema
• Retinal detachment
• Neovascularization
Prognosis
The prognosis of retinal hemorrhage largely depends on early detection and management of the underlying cause. In cases of hypertensive retinopathy, strict blood pressure control significantly improves outcomes and reduces recurrence risk.
Conclusion
Retinal hemorrhage is an important clinical finding that often reflects systemic vascular pathology. This case illustrates the critical role of early diagnosis, comprehensive evaluation, and timely management in preventing vision-threatening complications.
Control of systemic risk factors, particularly hypertension, remains the cornerstone of treatment. Regular ophthalmic follow-up and patient compliance are essential for long-term visual preservation.
Advancements in diagnostic imaging and therapeutic interventions continue to improve outcomes in patients with retinal vascular diseases.
References
- Wong TY, Mitchell P. Hypertensive retinopathy. https://pubmed.ncbi.nlm.nih.gov/12617828/
- Cheung N, et al. Diabetic retinopathy. https://pubmed.ncbi.nlm.nih.gov/23627796/
- StatPearls. Retinal Hemorrhage Overview. https://www.ncbi.nlm.nih.gov/books/NBK560777/
- American Academy of Ophthalmology. Retinal vascular diseases. https://www.aao.org/
- Hayreh SS. Retinal veinlusion. https://pubmed.ncbi.nlm.nih.gov/19671852/
- Spaide RF, et al. OCT in retinal diseases. https://pubmed.ncbi.nlm.nih.gov/20537310/
- Klein R, et al. Retinal vascular changes and systemic disease. https://pubmed.ncbi.nlm.nih.gov/16344421/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge