Osteomyelitis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Osteomyelitis is a serious infection of bone characterized by inflammatory destruction, necrosis, and new bone formation. It may arise from hematogenous spread, contiguous infection, or direct inoculation following trauma or surgery. Clinical manifestations vary depending on the acuity and underlying etiology, ranging from localized pain and swelling to systemic signs such as fever and malaise.
We present the case of a 45-year-old male with chronic osteomyelitis of the tibia following a neglected open fracture. The patient presented with persistent pain, swelling, and a discharging sinus over the affected site. Radiological and microbiological evaluations confirmed the diagnosis. A multidisciplinary management approach involving surgical debridement and targeted antibiotic therapy resulted in significant clinical improvement and infection control.
This case highlights the importance of early recognition, appropriate imaging, microbiological diagnosis, and combined medical-surgical management in optimizing outcomes in osteomyelitis.
Introduction
Osteomyelitis refers to infection and inflammation of bone and bone marrow, often resulting from bacterial invasion. It is broadly classified into acute, subacute, and chronic forms based on the duration and severity of infection. The most common causative organisms include Staphylococcus aureus, followed by gram-negative bacteria in certain populations.
The pathogenesis involves microbial colonization leading to inflammation, vascular compromise, and eventual bone necrosis. In chronic cases, sequestrum (dead bone) and involucrum (new bone formation) are hallmark features.
Osteomyelitis can arise through:
- Hematogenous spread (common in children)
- Contiguous spread from adjacent soft tissue infection
- Direct inoculation following trauma or surgery
Advancements in imaging modalities such as magnetic resonance imaging (MRI) and nuclear scans have improved early detection. Management requires prolonged antimicrobial therapy and often surgical intervention.
Case Report
Patient History
A 45-year-old male presented to the orthopedic clinic with complaints of persistent pain and swelling in the right leg for the past four months. The pain was dull, continuous, and exacerbated by weight-bearing.
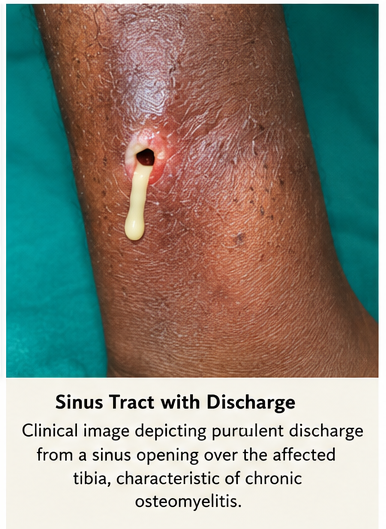
The patient reported a history of a road traffic accident six months prior, resulting in an open fracture of the right tibia. Initial treatment was received at a local facility, but follow-up care was irregular. Over time, he noticed intermittent purulent discharge from a sinus tract near the fracture site.
There was no history of diabetes mellitus, immunosuppression, or chronic illness. However, poor wound care and delayed treatment contributed to disease progression.
Clinical Examination
General Examination
The patient was afebrile at presentation but appeared mildly distressed due to pain. Vital signs were stable. No systemic signs of sepsis were noted.
Local Examination
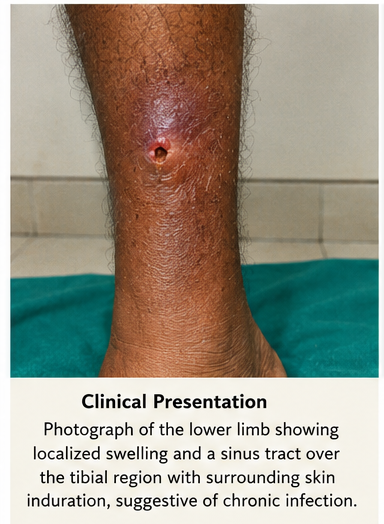
Inspection of the right leg revealed:
- Swelling over the mid-tibia
- A discharging sinus with purulent material
- Surrounding erythema and induration
Palpation demonstrated localized tenderness and warmth. Mild deformity was noted at the fracture site, suggesting possible non-union.
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation, the following conditions were considered:
- Chronic osteomyelitis (most likely)
- Infected non-union of fracture
- Soft tissue abscess
- Tubercular osteomyelitis
- Bone malignancy (less likely)
The presence of a sinus tract, history of trauma, and chronic symptoms strongly indicated osteomyelitis.
Investigations
Imaging Studies
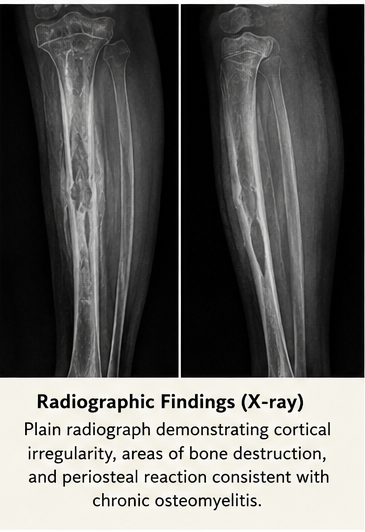
X-ray of the Right Leg:
Revealed cortical irregularity, areas of bone destruction, and periosteal reaction. A sequestrum was suspected.
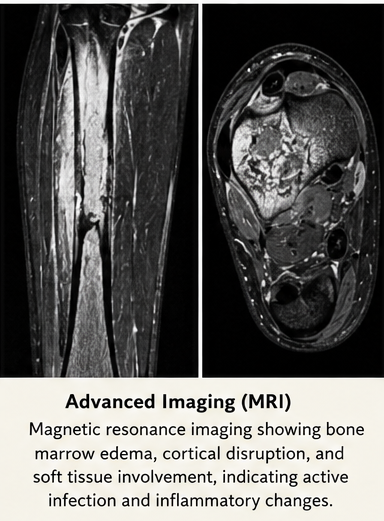
Magnetic Resonance Imaging (MRI):
Showed bone marrow edema, cortical disruption, and soft tissue involvement. The sinus tract extending to the bone confirmed chronic infection.
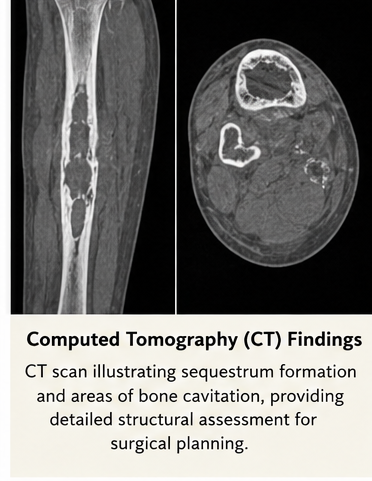
CT Scan (if required):
Provided detailed visualization of sequestrum and involucrum for surgical planning.
Laboratory Investigations
- Complete blood count: Mild leukocytosis
- Erythrocyte sedimentation rate (ESR): Elevated
- C-reactive protein (CRP): Elevated
- Blood cultures: Negative
Microbiological Analysis:
Culture of pus from the sinus tract revealed Staphylococcus aureus, sensitive to methicillin-based antibiotics.
Diagnosis
A definitive diagnosis of chronic osteomyelitis of the right tibia was established based on:
- Clinical findings (sinus tract, chronic pain)
- Imaging evidence of bone destruction
- Positive microbiological culture
The condition was categorized as post-traumatic chronic osteomyelitis.
Management and Outcome
Management Strategy
The treatment approach focused on:
- Eradication of infection
- Removal of necrotic bone
- Restoration of structural integrity
Medical Management
The patient was initiated on intravenous antibiotics based on culture sensitivity for a duration of two weeks, followed by oral antibiotics for an additional four weeks.
Anti-inflammatory medications were prescribed for pain control. Nutritional support and optimization of general health were emphasized.
Surgical Management
Surgical intervention included:
- Debridement of necrotic tissue
- Removal of sequestrum
- Irrigation of infected cavity
In selected areas, antibiotic-impregnated beads were placed to provide local antimicrobial therapy. Stabilization of the bone was achieved using external fixation due to compromised bone integrity.
Post-Treatment Course
The patient showed gradual improvement with reduction in pain and cessation of discharge. Wound healing progressed satisfactorily.
Follow-Up
At 1 Month
- Significant reduction in swelling
- No active discharge
- Improved mobility
At 3 Months
- ESR and CRP levels normalized
- Radiological evidence of bone healing
- Stable fixation
At 6 Months
- Complete resolution of infection
- Functional recovery achieved
- No recurrence of symptoms
Discussion
Pathophysiology
Osteomyelitis develops when pathogens invade bone tissue, leading to inflammation and vascular compromise. The resultant ischemia causes bone necrosis, forming sequestrum. Chronic inflammation stimulates new bone formation (involucrum), which may encase the infection and make eradication difficult.
Etiology and Risk Factors
Common risk factors include:
- Open fractures and trauma
- Surgical procedures
- Diabetes mellitus
- Peripheral vascular disease
- Immunocompromised states
In this case, trauma and inadequate initial management were key contributing factors.
Epidemiology
Osteomyelitis can occur at any age but varies in presentation:
- Children: Typically hematogenous
- Adults: Often due to trauma or surgery
Chronic osteomyelitis remains a significant healthcare burden due to prolonged treatment and risk of recurrence.
Clinical Manifestations
Symptoms depend on disease stage:
Acute Osteomyelitis:
- Fever
- Local pain and swelling
- Limited movement
Chronic Osteomyelitis:
- Persistent pain
- Sinus tract formation
- Intermittent discharge
- Bone deformity
The presented case demonstrated classic features of chronic disease.
Diagnostic Considerations
Diagnosis requires a combination of clinical, radiological, and microbiological evidence:
- Imaging:
- X-ray for structural changes
- MRI for early detection
- CT for surgical planning
- Laboratory Markers:
- ESR and CRP for inflammation
- Microbiology:
- Culture to identify causative organism
Early diagnosis is critical to prevent complications.
Treatment Considerations
Medical Therapy:
- Prolonged antibiotic therapy (4–6 weeks minimum)
- Tailored based on culture sensitivity
Surgical Intervention:
- Essential in chronic cases
- Removal of necrotic bone
- Drainage of abscess
Adjunctive Therapies:
- Local antibiotic delivery systems
- Bone grafting in selected cases
Emerging Therapies
Recent advances in osteomyelitis management include:
- Biofilm-targeted therapies
- Local antibiotic delivery using biodegradable carriers
- Stem cell-based bone regeneration
- Advanced imaging for early detection
Complications
If untreated or inadequately managed, osteomyelitis can lead to:
- Chronic infection
- Pathological fractures
- Septic arthritis
- Systemic sepsis
- Malignant transformation (rare, e.g., Marjolin ulcer)
Prognosis
The prognosis depends on:
- Early diagnosis
- Adequacy of surgical debridement
- Compliance with antibiotic therapy
Chronic osteomyelitis has a higher recurrence rate, but appropriate multidisciplinary management significantly improves outcomes.
Conclusion
Osteomyelitis is a complex and potentially debilitating condition requiring timely diagnosis and comprehensive management. This case underscores the importance of recognizing post-traumatic infections and initiating prompt treatment.
A combined approach involving targeted antibiotics and surgical intervention remains the cornerstone of therapy. Regular follow-up and patient compliance are essential to prevent recurrence and ensure long-term recovery.
Advancements in diagnostic tools and treatment modalities continue to enhance the management of osteomyelitis, improving both clinical outcomes and quality of life for affected patients.
References
- Lew DP, Waldvogel FA. Osteomyelitis. https://pubmed.ncbi.nlm.nih.gov/14557258/
- Calhoun JH, Manring MM. Adult osteomyelitis. https://pubmed.ncbi.nlm.nih.gov/19568028/
- Hatzenbuehler J, Pulling TJ. Diagnosis and management of osteomyelitis. https://pubmed.ncbi.nlm.nih.gov/23487380/
- Termaat MF, et al. The accuracy of diagnostic imaging for osteomyelitis. https://pubmed.ncbi.nlm.nih.gov/17556764/
- Mader JT, et al. Antimicrobial treatment of chronic osteomyelitis. https://pubmed.ncbi.nlm.nih.gov/10693988/
- Conterno LO, Turchi MD. Antibiotics for treating chronic osteomyelitis. https://pubmed.ncbi.nlm.nih.gov/23450541/
- Zimmerli W. Clinical practice: vertebral osteomyelitis. https://pubmed.ncbi.nlm.nih.gov/21226668/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge