Endometriosis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Endometriosis is a chronic estrogen-dependent gynecological disorder characterized by the presence of functional endometrial tissue outside the uterine cavity. It commonly affects women of reproductive age and presents with chronic pelvic pain, dysmenorrhea, dyspareunia, infertility, and menstrual irregularities. Delayed diagnosis may significantly impair quality of life and reproductive health.
We present the case of a 29-year-old female who presented with progressively worsening dysmenorrhea, chronic pelvic pain, and infertility for 3 years. Clinical examination, ultrasonography, and laparoscopic evaluation confirmed ovarian endometriosis with pelvic adhesions. The patient was managed with hormonal therapy, laparoscopic excision of endometriotic lesions, pain management, and fertility counseling, resulting in significant symptomatic improvement.
This case highlights the importance of early recognition, multidisciplinary management, and individualized treatment strategies in improving outcomes among patients with endometriosis.
Introduction
Endometriosis is a chronic inflammatory gynecological condition in which endometrial glands and stroma are found outside the uterine cavity. The disease most commonly involves the ovaries, pelvic peritoneum, uterosacral ligaments, pouch of Douglas, and fallopian tubes, although extra-pelvic involvement may also occur.
The condition affects approximately 10% of women of reproductive age and is strongly associated with chronic pelvic pain and infertility. Despite its high prevalence, diagnosis is often delayed because symptoms may overlap with other gynecological or gastrointestinal disorders.
Several mechanisms have been proposed in the pathogenesis of endometriosis, including retrograde menstruation, coelomic metaplasia, immune dysfunction, genetic susceptibility, and hormonal influences.
Important risk factors include:
• Early menarche
• Short menstrual cycles
• Heavy menstrual bleeding
• Family history of endometriosis
• Delayed childbearing
• Nulliparity
• Estrogen exposure
• Autoimmune predisposition
Common symptoms include:
• Severe dysmenorrhea
• Chronic pelvic pain
• Dyspareunia
• Infertility
• Pain during defecation or urination
• Menstrual irregularities
• Fatigue and reduced quality of life
Early diagnosis and individualized management are essential for symptom control, fertility preservation, and prevention of disease progression.
Case Report
Patient History
A 29-year-old married female presented to the gynecology outpatient department with:
• Severe dysmenorrhea for 5 years
• Chronic lower abdominal and pelvic pain
• Pain during sexual intercourse
• Difficulty conceiving for 3 years
• Increased pelvic discomfort during menstruation
The pain had progressively worsened over the past two years and significantly affected her daily activities and emotional well-being.
There was no history of:
• Previous pelvic surgery
• Tuberculosis
• Sexually transmitted infections
• Chronic systemic illness
• Malignancy
Family history revealed that the patient’s elder sister had previously been diagnosed with endometriosis.
Clinical Examination
General Examination
• Afebrile
• Pulse rate: 80/min
• Blood pressure: 116/74 mmHg
• Body mass index: 23 kg/m²
• Systemically stable
Gynecological Examination
Pelvic examination revealed:
• Tenderness in the posterior fornix
• Restricted uterine mobility
• Left adnexal tenderness
• Nodularity along uterosacral ligaments
• Mild pelvic fullness
No abnormal vaginal discharge or cervical lesions were noted.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Pelvic inflammatory disease
• Adenomyosis
• Ovarian cyst
• Irritable bowel syndrome
• Uterine fibroids
• Endometriosis
The cyclic nature of pain, infertility, dysmenorrhea, and pelvic tenderness strongly suggested endometriosis.
Investigations
Laboratory Findings
• Hemoglobin: Mild anemia detected
• White blood cell count: Normal
• CA-125: Mildly elevated
• Thyroid profile: Normal
• Hormonal profile: Within normal limits
Ultrasonography
Transvaginal ultrasonography revealed:
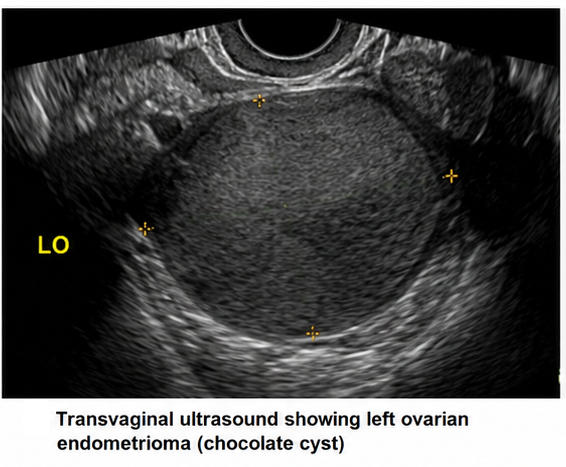
• Left ovarian endometrioma measuring 4 cm
• Thick-walled cyst with homogeneous low-level internal echoes
• Mild pelvic adhesions
Magnetic Resonance Imaging (MRI)
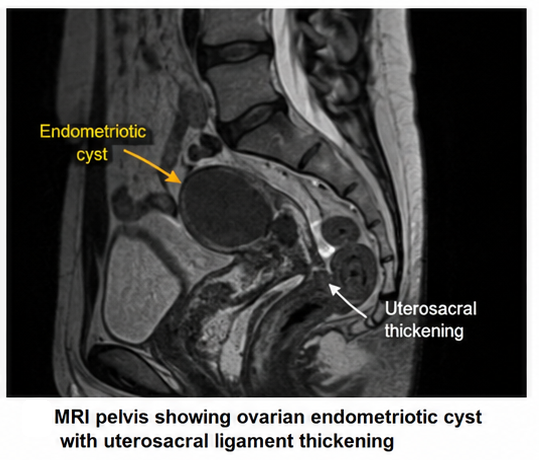
MRI pelvis demonstrated:
• Ovarian endometriotic cyst
• Pelvic adhesions
• Thickening of uterosacral ligaments
• Features suggestive of deep infiltrating endometriosis
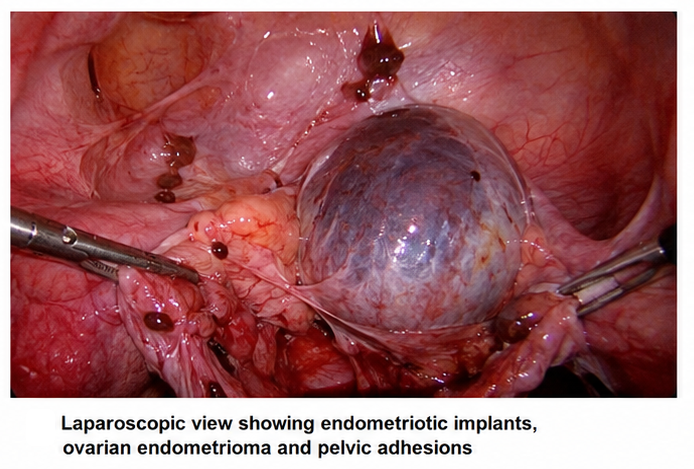
Diagnostic Laparoscopy
Laparoscopic evaluation revealed:
• Chocolate cyst involving left ovary
• Multiple endometriotic implants
• Dense pelvic adhesions
• Obliteration of pouch of Douglas
• Peritoneal inflammatory lesions
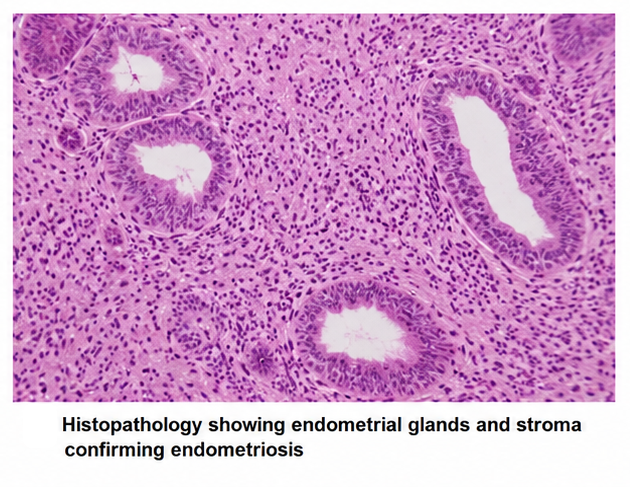
Histopathological examination confirmed endometrial glands and stroma outside the uterine cavity.
Diagnosis
Based on clinical presentation, imaging findings, laparoscopic evaluation, and histopathology, a diagnosis of Moderate-to-Severe Pelvic Endometriosis with Ovarian Endometrioma was established.
Management and Outcome
Initial Management
The patient was counseled regarding:
• Nature of the disease
• Chronicity and recurrence risk
• Fertility implications
• Lifestyle modifications
• Importance of long-term follow-up
Medical Management
The patient received:
• Nonsteroidal anti-inflammatory drugs (NSAIDs) for pain relief
• Combined oral contraceptive therapy
• Hormonal suppression therapy
• Iron supplementation for anemia
Surgical Management
Laparoscopic surgery was performed, including:
• Excision of endometriotic implants
• Adhesiolysis
• Ovarian cystectomy
• Restoration of pelvic anatomy
Follow-Up and Clinical Course
At 1 Month
• Significant reduction in pelvic pain
• Improved menstrual symptoms
• Better sleep and daily functioning
At 3 Months
• Marked reduction in dysmenorrhea
• Improvement in quality of life
• No significant recurrence of pelvic pain
At 6 Months
• Stable clinical condition
• Improved emotional well-being
• Fertility counseling continued
The patient remained under regular gynecological follow-up.
Discussion
Pathophysiology
Endometriosis is a multifactorial disease involving hormonal, immunological, inflammatory, and genetic mechanisms.
Important pathological mechanisms include:
• Retrograde menstruation with implantation of endometrial cells
• Chronic inflammatory response
• Estrogen-dependent proliferation
• Angiogenesis and fibrosis
• Adhesion formation
• Neurogenic inflammation causing chronic pain
The inflammatory microenvironment contributes significantly to pain, infertility, and disease progression.
Epidemiology
Important epidemiological features include:
• Affects nearly 1 in 10 women of reproductive age
• Commonly diagnosed between 25–35 years
• Frequently associated with infertility
• Strong familial predisposition
• Significant socioeconomic and psychological burden
Endometriosis remains underdiagnosed globally due to variability in symptoms and delayed recognition.
Clinical Manifestations
Common manifestations include:
• Dysmenorrhea
• Chronic pelvic pain
• Dyspareunia
• Infertility
• Dyschezia
• Menorrhagia
• Fatigue
Commonly affected anatomical sites include:
• Ovaries
• Pelvic peritoneum
• Uterosacral ligaments
• Rectovaginal septum
• Fallopian tubes
Diagnostic Considerations
Diagnosis is often delayed because symptoms may mimic other gynecological or gastrointestinal conditions.
Important diagnostic modalities include:
- Pelvic examination
- Transvaginal ultrasonography
- MRI pelvis
- Serum CA-125
- Diagnostic laparoscopy with biopsy
Laparoscopy remains the gold standard for definitive diagnosis.
Treatment Modalities
Conservative Management
Supportive measures include:
• Lifestyle modification
• Exercise and stress reduction
• Nutritional counseling
• Psychological support
Pharmacological Therapy
Medical treatment options include:
• NSAIDs
• Combined oral contraceptives
• Progestins
• Gonadotropin-releasing hormone agonists
• Aromatase inhibitors
• Hormonal suppression therapy
Surgical Management
Surgery may be required for:
• Severe pain
• Large endometriomas
• Adhesions
• Infertility
• Failure of medical therapy
Laparoscopic excision remains the preferred surgical approach.
Complications
Potential complications include:
• Chronic pelvic pain syndrome
• Infertility
• Ovarian cyst rupture
• Adhesion formation
• Bowel and bladder involvement
• Psychological distress
• Reduced quality of life
Delayed treatment may result in progressive disease and reproductive complications.
Prognosis
The prognosis depends upon:
• Severity of disease
• Early diagnosis
• Response to hormonal therapy
• Surgical outcomes
• Fertility status
• Long-term follow-up adherence
Although recurrence is common, early multidisciplinary management significantly improves symptom control and quality of life.
Conclusion
Endometriosis is a chronic inflammatory gynecological disorder that can significantly affect reproductive health, psychological well-being, and quality of life if left untreated. Early recognition of dysmenorrhea, chronic pelvic pain, infertility, and cyclic symptoms is essential for timely diagnosis.
This case highlights the importance of imaging evaluation, laparoscopic confirmation, individualized hormonal therapy, and surgical management in achieving favorable clinical outcomes. Long-term follow-up, fertility counseling, and patient education remain critical components in the comprehensive management of endometriosis.
References
- Zondervan KT, Becker CM, Missmer SA. Endometriosis. https://pubmed.ncbi.nlm.nih.gov/30355456/
- Giudice LC. Clinical practice. Endometriosis. https://pubmed.ncbi.nlm.nih.gov/16421367/
- Burney RO, Giudice LC. Pathogenesis and pathophysiology of endometriosis. https://pubmed.ncbi.nlm.nih.gov/22085724/
- Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease. https://pubmed.ncbi.nlm.nih.gov/31672535/
- American College of Obstetricians and Gynecologists. Endometriosis FAQ. https://www.acog.org/womens-health/faqs/endometriosis
- World Health Organization. Endometriosis Fact Sheet. https://www.who.int/news-room/fact-sheets/detail/endometriosis
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Scientists hail the cervical cancer treatment as the most remarkable breakthrough in 20 years.
2.
Researchers use AI to monitor side effects of chemotherapy and support families dealing with pediatric cancer.
3.
Study finds 20 minutes of mindful breathing can rapidly reduce intensity of cancer pain
4.
Report suggests a big improvement in lung cancer survival
5.
The clinical trial of ENZAMET shows promise as a treatment for prostate cancer.
1.
Clinical Analysis of Prostate Cancer
2.
All You Need to Know About Mesna: The Ultimate Guide
3.
The Unfolding Revolution of Precision Medicine, Immunotherapy, and Digital Transformation in Medical Oncology 2025
4.
The Latest Research on Basal Cell Carcinoma: New Developments in Diagnosis and Cure
5.
Early-Onset GI Cancers: Screening, AI Innovations & Research Advances 2025
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Understanding Early Relapse in B-cell ALL: Rates, Risks, and Common Sites
2.
Newer Immunotherapies for Myeloma- A Comprehensive Overview
3.
Targeting Oncologic Drivers: A New Approach to Lung Cancer Treatment
4.
An Eagles View - Evidence-based Discussion on Iron Deficiency Anemia- Panel Discussion- Part II
5.
Iron Deficiency Anemia: Ferric Maltol As a New Treatment Option- Summarization of the New Perspective

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge