Laser Peripheral Iridotomy: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
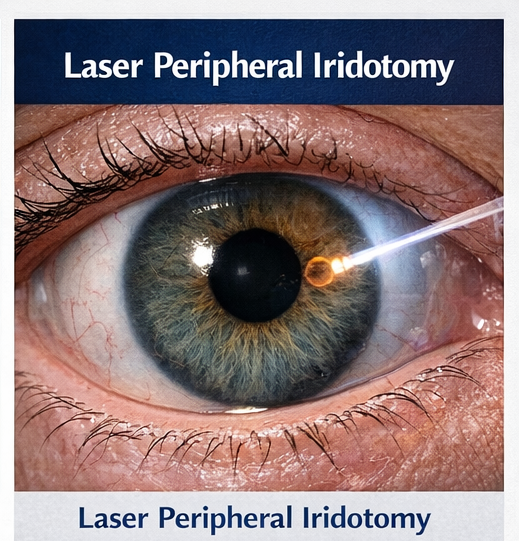
Acute primary angle-closure glaucoma (PACG) is an ophthalmic emergency characterized by sudden elevation of intraocular pressure (IOP) due to pupillary block and iridotrabecular apposition, leading to rapid visual deterioration if not promptly treated. Laser peripheral iridotomy (LPI) creates an alternate aqueous humor pathway, relieving pupillary block and preventing recurrent angle closure. Clinical presentation includes acute ocular pain, headache, nausea, blurred vision with halos, conjunctival congestion, corneal edema, and mid-dilated fixed pupil. Diagnosis is established through tonometry, slit-lamp biomicroscopy, gonioscopy, and optic nerve evaluation. Prompt medical IOP lowering followed by definitive LPI is the standard of care to preserve vision and prevent optic neuropathy. We report a case of acute angle-closure managed with urgent medical therapy and bilateral prophylactic LPI, highlighting presentation, diagnostic evaluation, procedural management, and short-term outcomes. Early recognition, rapid IOP control, and timely iridotomy are critical to prevent permanent glaucomatous damage.
Introduction
Primary angle-closure disease is a major cause of irreversible blindness, particularly in Asian populations and elderly hyperopic individuals. Pupillary block with forward bowing of the peripheral iris results in acute or intermittent angle closure, abrupt IOP elevation, corneal edema, and optic nerve ischemia. Laser peripheral iridotomy addresses the upstream mechanism by equalizing pressure between posterior and anterior chambers, opening the angle and preventing recurrence.
Delayed diagnosis is associated with optic nerve damage, peripheral anterior synechiae formation, and chronic angle-closure glaucoma. A high index of suspicion, rapid medical stabilization, and definitive laser intervention are essential determinants of visual prognosis.
Case Report
Patient History
A 58-year-old female presented to the emergency ophthalmology service with sudden onset severe pain in the right eye, headache, nausea, and blurred vision with colored halos for 12 hours. She reported intermittent episodes of ocular discomfort over the past month, precipitated in dim light. There was no history of trauma or prior ocular surgery. Medical history included controlled hypertension. Family history was positive for glaucoma in a first-degree relative.
Clinical Examination
On examination, visual acuity was counting fingers at 2 meters in the right eye and 6/9 in the left eye. The right eye showed conjunctival congestion, corneal edema, shallow anterior chamber, and a mid-dilated sluggish pupil. The left eye had a shallow anterior chamber peripherally. Intraocular pressure measured by applanation tonometry was 48 mmHg in the right eye and 20 mmHg in the left eye. Fundoscopy of the right eye was limited by corneal edema; the left optic disc showed a cup-to-disc ratio of 0.4 with healthy neuroretinal rim.
Clinical Evaluation
Differential Diagnosis
- Acute primary angle-closure glaucoma
- Secondary angle closure (lens-induced)
- Uveitic glaucoma
- Neovascular glaucoma
- Acute anterior uveitis
Investigations
- Tonometry: Markedly elevated IOP in the affected eye
- Slit-lamp biomicroscopy: Corneal edema, shallow anterior chamber, mid-dilated pupil
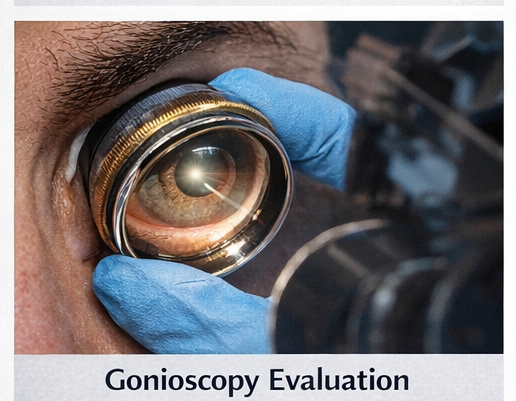
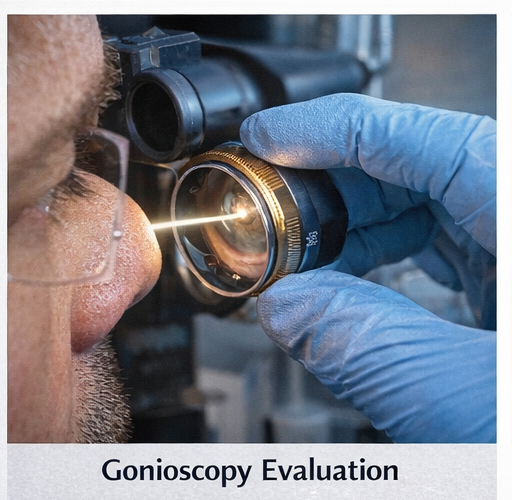
- Gonioscopy (after IOP reduction): Occludable angles bilaterally with peripheral anterior synechiae in the right eye
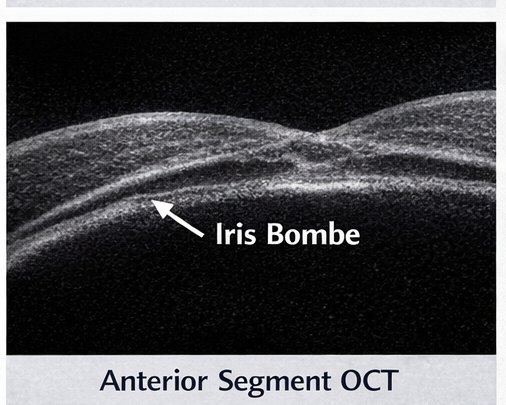
- Anterior segment OCT: Iris bombe configuration with narrow angles
- Optic nerve assessment (post-edema resolution): Early glaucomatous cupping in the right eye
- Visual fields (baseline): Early paracentral defects in the right eye
Findings were consistent with acute primary angle closure in the right eye with occludable angles in the fellow eye.
Management and Outcome
Management Strategy
The patient was admitted for urgent IOP reduction and definitive laser therapy.
Immediate medical therapy:
- Topical beta-blocker, alpha-agonist, and carbonic anhydrase inhibitor
- Systemic acetazolamide
- Hyperosmotic agent (oral glycerol)
- Topical steroid to reduce inflammation
- Topical pilocarpine initiated after partial IOP reduction
Definitive treatment:
- Laser peripheral iridotomy to the right eye once corneal clarity improved
- Prophylactic laser peripheral iridotomy to the left eye due to occludable angles
Supportive care and monitoring:
- Analgesia and antiemetics
- Serial IOP measurements
- Post-laser anti-inflammatory drops
- Patient education regarding symptoms of recurrence
Follow-Up and Outcome
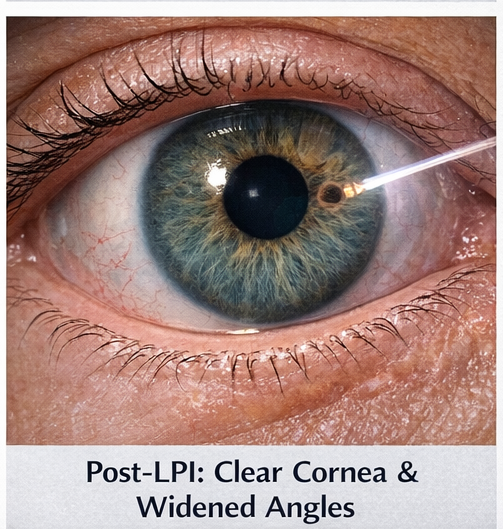
Within 24 hours, IOP reduced to 16 mmHg in the right eye with resolution of corneal edema and significant symptomatic relief. Post-LPI gonioscopy demonstrated widened angles in both eyes. At 2-week follow-up, visual acuity improved to 6/12 in the right eye and 6/9 in the left eye. At 2 months, IOP remained controlled on topical monotherapy, with stable optic nerve appearance and no recurrent angle-closure episodes. The patient was counseled regarding long-term follow-up and risk of chronic angle-closure glaucoma.
Discussion
Acute angle-closure glaucoma constitutes a true ophthalmic emergency in which rapid intraocular pressure (IOP) elevation precipitates corneal edema, ischemia of the optic nerve head, and acute visual compromise, necessitating immediate pressure-lowering measures followed by definitive elimination of the underlying mechanism of pupillary block. Initial stabilization with topical and systemic hypotensive agents, cycloplegia, and anti-inflammatory therapy is essential to clear corneal edema, improve visualization, and create safe conditions for definitive laser intervention. Delay in prompt IOP control not only exacerbates optic nerve ischemia but also promotes the formation of peripheral anterior synechiae, predisposing to chronic angle-closure glaucoma and refractory long-term pressure elevation.
Laser peripheral iridotomy remains the first-line definitive intervention, re-establishing physiological aqueous flow between the posterior and anterior chambers, relieving iris bombe, and preventing recurrent angle closure and progression to chronic glaucomatous optic neuropathy. In anatomically predisposed eyes, prophylactic iridotomy of the fellow eye is strongly recommended to mitigate the high risk of bilateral involvement and avert future acute attacks. However, iridotomy alone may be insufficient in eyes with plateau iris configuration, extensive synechial closure, or lens-related mechanisms, necessitating adjunctive strategies such as argon laser peripheral iridoplasty or lens extraction in selected cases.
Long-term surveillance is mandatory to detect residual appositional or synechial angle closure, persistent or recurrent IOP elevation, progressive optic nerve damage, and visual field loss. Multimodal anterior segment imaging, including anterior segment optical coherence tomography and ultrasound biomicroscopy, in conjunction with serial gonioscopy, provides robust phenotyping, risk stratification, and therapeutic guidance across the disease continuum. Structured follow-up integrating optic nerve head and retinal nerve fiber layer imaging, perimetry, and longitudinal IOP profiling is critical to ensure durable disease control and preservation of visual function.
Conclusion
Laser peripheral iridotomy is a sight-saving, mechanism-targeted intervention in acute primary angle-closure disease, directly relieving pupillary block and restoring physiological aqueous humor flow between the posterior and anterior chambers. By eliminating the pressure gradient that drives iris bombe and iridotrabecular apposition, timely iridotomy halts the cascade leading to sustained intraocular pressure (IOP) elevation, corneal decompensation, and ischemic optic neuropathy. Early recognition of prodromal symptoms—such as intermittent ocular pain, headache, halos around lights, and blurred vision—enables prompt triage, rapid pharmacologic IOP reduction, and definitive laser therapy before irreversible structural damage occurs.
In high-risk eyes with anatomically narrow angles, bilateral iridotomy significantly reduces the risk of recurrent angle closure and progression to chronic angle-closure glaucoma with peripheral anterior synechiae formation. However, iridotomy does not obviate the need for longitudinal surveillance. Structured follow-up with periodic gonioscopy, optic nerve head and retinal nerve fiber layer assessment, visual field testing, and IOP monitoring is essential to detect residual or progressive angle closure, post-laser inflammation, and conversion to chronic disease requiring adjunctive medical or surgical escalation.
References
- The Lancet – Glaucoma and primary angle-closure disease overview.
- The New England Journal of Medicine – Acute angle-closure glaucoma management.
- Ophthalmology – Laser peripheral iridotomy outcomes in angle-closure disease.
- American Journal of Ophthalmology – Anterior segment imaging in angle-closure glaucoma.
- Cochrane Database of Systematic Reviews – Interventions for primary angle-closure glaucoma.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Scientists hail the cervical cancer treatment as the most remarkable breakthrough in 20 years.
2.
Researchers use AI to monitor side effects of chemotherapy and support families dealing with pediatric cancer.
3.
Study finds 20 minutes of mindful breathing can rapidly reduce intensity of cancer pain
4.
Report suggests a big improvement in lung cancer survival
5.
The clinical trial of ENZAMET shows promise as a treatment for prostate cancer.
1.
Clinical Analysis of Prostate Cancer
2.
All You Need to Know About Mesna: The Ultimate Guide
3.
The Unfolding Revolution of Precision Medicine, Immunotherapy, and Digital Transformation in Medical Oncology 2025
4.
The Latest Research on Basal Cell Carcinoma: New Developments in Diagnosis and Cure
5.
Early-Onset GI Cancers: Screening, AI Innovations & Research Advances 2025
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Understanding Early Relapse in B-cell ALL: Rates, Risks, and Common Sites
2.
Newer Immunotherapies for Myeloma- A Comprehensive Overview
3.
Targeting Oncologic Drivers: A New Approach to Lung Cancer Treatment
4.
An Eagles View - Evidence-based Discussion on Iron Deficiency Anemia- Panel Discussion- Part II
5.
Iron Deficiency Anemia: Ferric Maltol As a New Treatment Option- Summarization of the New Perspective

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge