Tinea Versicolor: Clinical Presentation, Diagnostic Challenges, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Tinea versicolor (pityriasis versicolor) is a common superficial fungal infection of the skin caused by Malassezia species, characterized by hypo- or hyperpigmented macules with fine scaling, predominantly affecting the trunk and proximal upper limbs. Although benign, the condition often leads to cosmetic concern and recurrent disease, especially in warm and humid climates. Diagnosis is usually clinical but may be challenging due to resemblance to other hypopigmentary dermatoses. We report a confirmed case of tinea versicolor in a young adult male presenting with multiple asymptomatic hypopigmented patches over the chest and back. This case highlights the clinical presentation, diagnostic challenges, confirmatory investigations, treatment approach, and clinical outcome. The report emphasizes the importance of clinical recognition, appropriate mycological confirmation when needed, patient counseling regarding recurrence, and adherence to antifungal therapy to achieve sustained remission.
Introduction
Tinea versicolor is a superficial cutaneous mycosis caused by lipophilic yeasts of the genus Malassezia, which are part of the normal skin flora. Under predisposing conditions such as warm and humid climate, excessive sweating, oily skin, immunosuppression, and malnutrition, these commensal organisms convert to a pathogenic mycelial form, leading to characteristic pigmentary changes of the skin.
The disease is prevalent in tropical and subtropical regions, with peak incidence in adolescents and young adults. Lesions commonly involve the upper trunk, neck, shoulders, and proximal upper limbs. Although the condition is non-contagious and medically benign, it often causes significant cosmetic distress and psychosocial impact. Recurrence is common, reflecting persistence of the organism in sebaceous-rich areas.
Diagnosis is primarily clinical but may be supported by Wood’s lamp examination and potassium hydroxide (KOH) microscopy. This case report illustrates a typical presentation of tinea versicolor, discusses diagnostic pitfalls, management strategies, and clinical outcome, and highlights the importance of patient education regarding recurrence prevention.
Case Report
Patient History
A 26-year-old man presented to the dermatology outpatient clinic with a 3-month history of multiple asymptomatic, progressively increasing light-colored patches over the upper chest, back, and shoulders. The lesions were more noticeable after sun exposure. The patient reported mild occasional itching, especially after sweating. There was no history of pain, discharge, or systemic symptoms such as fever or weight loss.
The patient was a college student residing in a hostel in a hot and humid environment and reported excessive sweating. There was no history of diabetes mellitus, long-term steroid use, or immunosuppression. No similar lesions were noted among close contacts. He had previously used over-the-counter moisturizers without improvement.
Clinical Examination
Cutaneous examination revealed multiple, well-demarcated, hypopigmented macules and patches with fine branny scaling distributed over the upper chest, interscapular region, and proximal upper arms. The lesions coalesced in some areas, forming larger patches. Stretching of the skin accentuated the fine scaling (evoked scale sign).

There were no signs of inflammation, secondary infection, or scarring. Hair, nails, and mucous membranes were normal. No lymphadenopathy was noted.
Clinical Evaluation
Differential Diagnosis
The differential diagnoses included:
- Tinea versicolor
- Vitiligo
- Pityriasis alba
- Post-inflammatory hypopigmentation
- Early leprosy
The presence of fine scaling, truncal distribution, seasonal exacerbation, and absence of sensory loss favored tinea versicolor.
Investigations
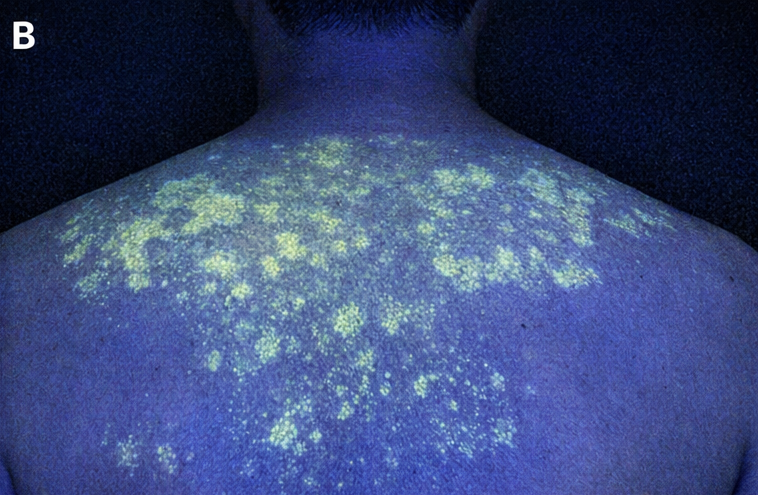
Wood’s Lamp Examination
Wood’s lamp examination demonstrated yellowish-green fluorescence over the affected areas, suggestive of Malassezia infection.
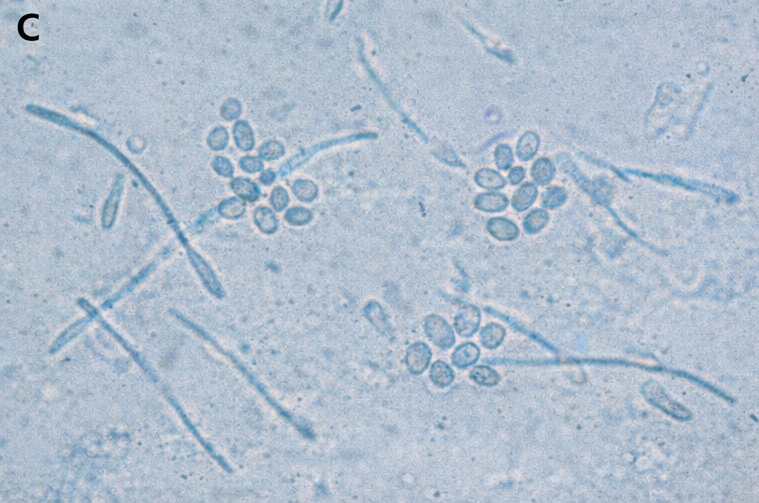
Microscopy
Skin scrapings from the lesions were examined with 10% potassium hydroxide (KOH) preparation, revealing short hyphae and clusters of spores in the characteristic “spaghetti and meatballs” appearance, confirming the diagnosis of tinea versicolor.
Routine blood investigations were not indicated, as the patient had no features suggestive of immunodeficiency.
Diagnosis
Based on clinical features and confirmatory KOH microscopy, a definitive diagnosis of tinea versicolor was established.
Management and Outcome
Management Strategy
The patient was treated with topical antifungal therapy consisting of ketoconazole 2% shampoo applied over the affected areas and left for 10 minutes before rinsing, once daily for 5 days. In addition, ketoconazole 2% cream was advised twice daily for 2 weeks over persistent lesions.

The patient was counseled regarding the benign nature of the condition, high likelihood of recurrence, and the delayed repigmentation even after successful eradication of the fungus. Preventive measures, including regular bathing after sweating, avoiding excessive oil-based products, and wearing loose, breathable clothing, were advised.
As the disease extent was moderate and the patient was immunocompetent, systemic antifungal therapy was not initiated.
Follow-Up and Outcome
At 4-week follow-up, the patient reported complete resolution of scaling and itching. The lesions showed gradual repigmentation, though some hypopigmented patches persisted, consistent with post-treatment pigmentary normalization.
At 3-month follow-up, no new lesions were observed. The patient was advised monthly prophylactic use of ketoconazole shampoo during the summer months to prevent recurrence.
Discussion
Tinea versicolor is a common superficial mycosis in tropical climates, frequently affecting young adults due to increased sebaceous gland activity and sweating. The disease results from overgrowth of Malassezia species and interference with normal melanocyte function, leading to hypopigmented or hyperpigmented lesions.
Clinical diagnosis is often straightforward; however, conditions such as vitiligo and pityriasis alba may mimic tinea versicolor, leading to misdiagnosis. Wood’s lamp examination and KOH microscopy provide rapid and inexpensive diagnostic confirmation.
Topical antifungals remain the first-line therapy for localized or moderate disease, while systemic azoles are reserved for extensive or recurrent cases. Despite effective treatment, recurrence rates are high, necessitating patient education and preventive strategies. Persistent hypopigmentation after treatment reflects melanocyte suppression and may take weeks to months to resolve, which should be explained to patients to avoid premature treatment failure assumptions.
Conclusion
Tinea versicolor is a common, benign, and treatable superficial fungal infection with characteristic clinical and microscopic features. This case highlights the importance of accurate diagnosis, appropriate topical antifungal therapy, and patient counseling regarding recurrence and delayed pigment normalization. Early recognition and preventive measures can significantly reduce disease recurrence and improve patient satisfaction.
References
- Gupta AK, Batra R, Bluhm R, Boekhout T, Dawson TL Jr. Skin diseases associated with Malassezia species. J Am Acad Dermatol. 2004;51(5):785–98.
- Kaur I, Handa S. Pityriasis versicolor: A clinical and epidemiological study. Indian J Dermatol Venereol Leprol. 2004;70(6):344–6.
- Hay RJ, Ashbee HR. Fungal infections. In: Griffiths CEM, Barker J, Bleiker T, Chalmers R, Creamer D, editors. Rook’s Textbook of Dermatology. 9th ed. Wiley-Blackwell; 2016.
- Gupta AK, Lyons DCA. The role of antifungal therapy in pityriasis versicolor. J Eur Acad Dermatol Venereol. 2014;28(9):1125–31.
- Faergemann J. Management of seborrheic dermatitis and pityriasis versicolor. Am J Clin Dermatol. 2000;1(2):75–80.
- Crespo-Erchiga V, Florencio VD. Malassezia yeasts and pityriasis versicolor. Curr Opin Infect Dis. 2006;19(2):139–47.
- Gaitanis G, Bassukas ID, Velegraki A. The role of Malassezia in skin diseases. J Am Acad Dermatol. 2012;67(3):e1–19.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Scientists hail the cervical cancer treatment as the most remarkable breakthrough in 20 years.
2.
Researchers use AI to monitor side effects of chemotherapy and support families dealing with pediatric cancer.
3.
Study finds 20 minutes of mindful breathing can rapidly reduce intensity of cancer pain
4.
Report suggests a big improvement in lung cancer survival
5.
The clinical trial of ENZAMET shows promise as a treatment for prostate cancer.
1.
Clinical Analysis of Prostate Cancer
2.
All You Need to Know About Mesna: The Ultimate Guide
3.
The Unfolding Revolution of Precision Medicine, Immunotherapy, and Digital Transformation in Medical Oncology 2025
4.
The Latest Research on Basal Cell Carcinoma: New Developments in Diagnosis and Cure
5.
Early-Onset GI Cancers: Screening, AI Innovations & Research Advances 2025
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Understanding Early Relapse in B-cell ALL: Rates, Risks, and Common Sites
2.
Newer Immunotherapies for Myeloma- A Comprehensive Overview
3.
Targeting Oncologic Drivers: A New Approach to Lung Cancer Treatment
4.
An Eagles View - Evidence-based Discussion on Iron Deficiency Anemia- Panel Discussion- Part II
5.
Iron Deficiency Anemia: Ferric Maltol As a New Treatment Option- Summarization of the New Perspective

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge