Pancreatic Calcifications: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Pancreatic calcifications are a hallmark feature of chronic pancreatitis, representing long-standing inflammation, fibrosis, and ductal obstruction. These calcifications are commonly associated with alcohol-related chronic pancreatitis but may also arise from idiopathic, hereditary, or metabolic causes. The condition leads to progressive pancreatic insufficiency, chronic abdominal pain, and metabolic complications such as diabetes mellitus.
We report the case of a 48-year-old male presenting with recurrent abdominal pain, weight loss, and steatorrhea. Radiological imaging revealed extensive pancreatic calcifications consistent with chronic calcific pancreatitis. The patient was managed with a combination of medical therapy, pancreatic enzyme supplementation, and lifestyle modification, resulting in symptomatic improvement and stabilization of disease progression.
This case underscores the importance of early recognition, appropriate imaging, and multidisciplinary management to reduce complications and improve quality of life in patients with pancreatic calcifications.
Introduction
Pancreatic calcifications are most commonly observed in chronic pancreatitis and are indicative of advanced disease. These calcifications arise due to prolonged inflammation, protein plug formation, and subsequent deposition of calcium salts within pancreatic ducts and parenchyma.
Chronic pancreatitis is characterized by irreversible structural damage, leading to impairment of both exocrine and endocrine pancreatic function. The condition is frequently associated with significant morbidity due to chronic pain, malabsorption, and diabetes.
The pathophysiology involves:
• Chronic inflammation leading to fibrosis and ductal distortion
• Formation of protein plugs within pancreatic ducts
• Progressive calcium deposition resulting in calcifications
• Loss of functional pancreatic tissue
Key etiological factors include:
• Chronic alcohol consumption (most common cause)
• Idiopathic pancreatitis
• Genetic mutations (e.g., PRSS1, SPINK1)
• Hyperparathyroidism and hypercalcemia
• Obstructive causes such as pancreatic duct strictures
Clinically, patients may present with:
• Recurrent epigastric abdominal pain
• Steatorrhea due to fat malabsorption
• Weight loss
• Diabetes mellitus (secondary pancreatic insufficiency)
Due to its progressive nature, early diagnosis is often challenging.
Case Report
Patient History
A 48-year-old male presented with:
• Recurrent upper abdominal pain for 4 years
• Pain radiating to the back, aggravated after meals
• Significant weight loss (~8 kg over 6 months)
• Frequent loose, greasy stools suggestive of steatorrhea
Additional history revealed:
• Chronic alcohol consumption for over 15 years
• Loss of appetite and fatigue
There was no history of gallstones, trauma, or prior pancreatic surgery. No family history of pancreatic disease was noted.
Clinical Examination
On examination:
• Mild epigastric tenderness
• Evidence of muscle wasting
• No jaundice or palpable abdominal mass
Vital signs:
• Blood pressure: 130/85 mmHg
• Body mass index (BMI): 22 kg/m²
Systemic examination was otherwise unremarkable.
Clinical Evaluation
Differential Diagnosis
The following conditions were considered:
• Chronic calcific pancreatitis
• Pancreatic carcinoma
• Recurrent acute pancreatitis
• Peptic ulcer disease
• Gallstone-related pancreatic disease
Chronicity of symptoms and steatorrhea strongly favored chronic pancreatitis.
Investigations
Biochemical Assessment
• Serum amylase and lipase: mildly elevated
• Fasting blood glucose: elevated
• HbA1c: consistent with diabetes mellitus
• Serum calcium: normal
• Liver function tests: within normal limits
Stool Analysis
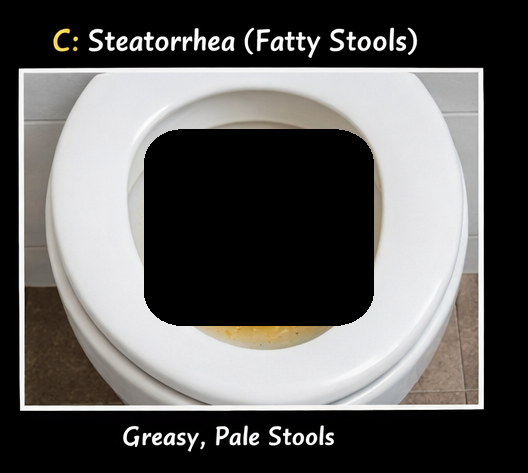
• Increased fecal fat confirming steatorrhea
Imaging
Abdominal imaging revealed:
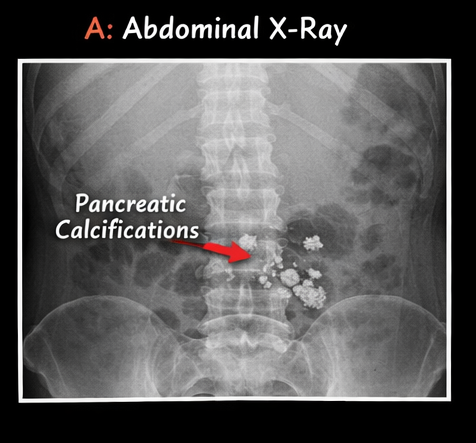
• X-ray abdomen: multiple calcifications in the pancreatic region
• Ultrasound: heterogeneous pancreas with echogenic foci
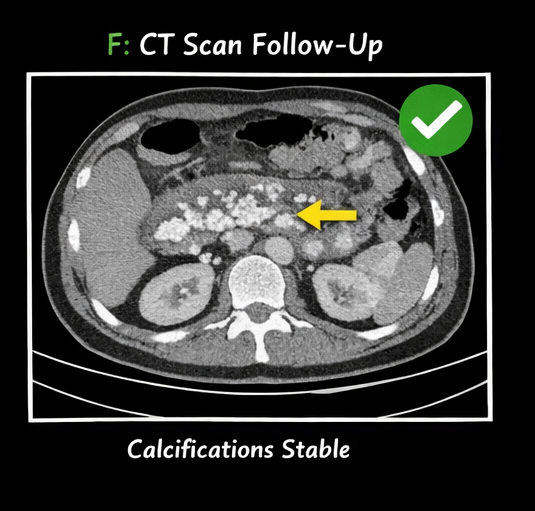
• CT scan (contrast-enhanced):
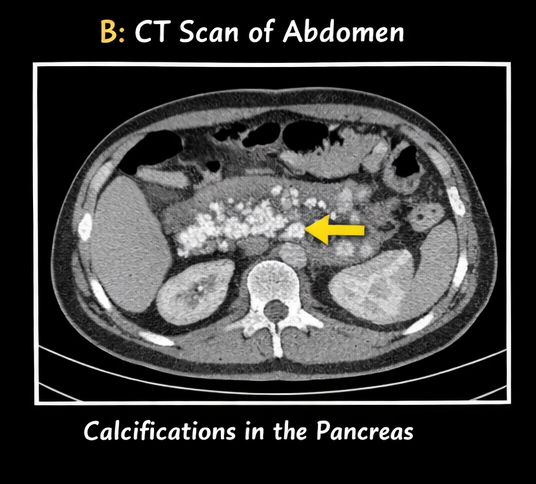
- Multiple intraductal and parenchymal calcifications
- Dilated pancreatic duct
- Atrophic pancreatic parenchyma
These findings confirmed chronic calcific pancreatitis.
Diagnosis
Based on clinical history, biochemical findings, and imaging evidence, a diagnosis of chronic calcific pancreatitis with pancreatic insufficiency was established.
Management and Outcome
Management Strategy
A multidisciplinary approach involving gastroenterologists, nutritionists, and pain specialists was adopted.
Medical Management
• Pancreatic enzyme replacement therapy (PERT)
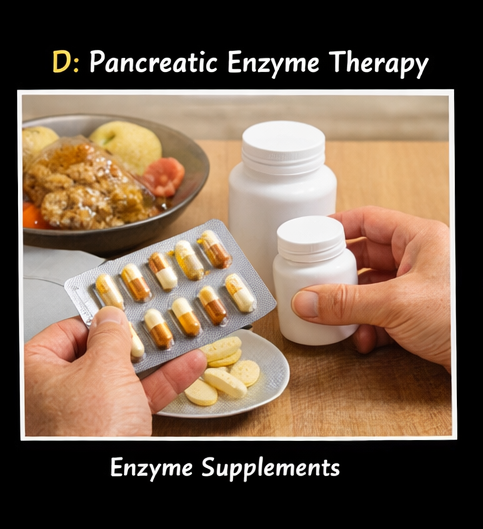
• Analgesics for pain control
• Proton pump inhibitors to enhance enzyme efficacy
Lifestyle Modification
• Complete abstinence from alcohol
• Dietary modification (low-fat, high-protein diet)
• Nutritional supplementation (fat-soluble vitamins A, D, E, K)
Glycemic Control
• Initiation of oral hypoglycemic agents
• Regular monitoring for pancreatic diabetes
Follow-Up and Outcome
At 1 month:
• Reduction in abdominal pain
• Improved appetite
At 3 months:
• Decrease in steatorrhea
• Weight stabilization
At 6 months:
• Better glycemic control
• Improved nutritional status
At 12 months:
• No progression of calcifications
• Significant improvement in quality of life
Discussion
Pathophysiology
Pancreatic calcifications develop as a result of prolonged inflammation leading to:
• Protein precipitation within pancreatic ducts
• Ductal obstruction
• Calcium salt deposition
These changes contribute to:
• Exocrine insufficiency → malabsorption
• Endocrine insufficiency → diabetes mellitus
Diagnostic Challenges
Diagnosis may be delayed due to:
• Non-specific abdominal symptoms
• Overlap with other gastrointestinal disorders
Key diagnostic tools include:
• CT scan (gold standard for calcification detection)
• Ultrasound for initial evaluation
• Endoscopic ultrasound (EUS) for early disease
Treatment Considerations
Medical Therapy
• First-line for symptom control
• Includes enzyme replacement and analgesics
Endoscopic Management
Indicated for:
• Ductal obstruction
• Large intraductal stones
Options include:
• ERCP with stone extraction
• Pancreatic duct stenting
Surgical Management
Reserved for refractory cases:
• Pancreatic duct drainage procedures (e.g., Puestow procedure)
• Resection surgeries
Complications
Potential complications include:
• Chronic pain syndrome
• Diabetes mellitus
• Pancreatic pseudocysts
• Pancreatic cancer (in long-standing cases)
• Malnutrition
Prognosis
Prognosis depends on:
• Alcohol cessation
• Degree of pancreatic damage
• Early initiation of therapy
With appropriate management, disease progression can be slowed and quality of life significantly improved.
Conclusion
Pancreatic calcifications are a defining feature of chronic pancreatitis and indicate advanced pancreatic damage. This case highlights the importance of recognizing key clinical features such as chronic abdominal pain, steatorrhea, and weight loss.
Imaging plays a pivotal role in diagnosis, with CT scans providing definitive evidence of calcifications. Adjunct modalities such as ultrasound and endoscopic ultrasound can further aid in early detection and assessment of disease severity. Management requires a comprehensive approach including enzyme replacement, pain control, lifestyle modification, and metabolic management.
In addition, strict alcohol abstinence and nutritional optimization are essential components of long-term care. Regular monitoring for endocrine insufficiency, particularly diabetes mellitus, is crucial in preventing metabolic complications. Patients should also be evaluated periodically for structural complications such as pseudocysts or ductal obstruction.
Early diagnosis and sustained intervention are critical in preventing complications and improving long-term outcomes in patients with chronic calcific pancreatitis. A multidisciplinary approach significantly enhances disease control, symptom relief, and overall quality of life.
References
- Whitcomb DC. Chronic pancreatitis: an update. Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/16530512/
- Yadav D, Lowenfels AB. The epidemiology of pancreatitis. Gastroenterology. https://pubmed.ncbi.nlm.nih.gov/18395063/
- Braganza JM, Lee SH, McCloy RF, McMahon MJ. Chronic pancreatitis. Lancet. https://pubmed.ncbi.nlm.nih.gov/11214196/
- Conwell DL, Lee LS, Yadav D, et al. American Pancreatic Association guidelines. https://pubmed.ncbi.nlm.nih.gov/25830654/
- Stevens T, Conwell DL, Zuccaro G. Pathogenesis of chronic pancreatitis. https://pubmed.ncbi.nlm.nih.gov/15825035/
- Löhr JM, Dominguez-Muñoz E, Rosendahl J, et al. United European Gastroenterology guidelines. https://pubmed.ncbi.nlm.nih.gov/27697421/
- Drewes AM, Bouwense SA, Campbell CM, et al. Pain in chronic pancreatitis. https://pubmed.ncbi.nlm.nih.gov/25062878/
- Hart PA, Conwell DL. Chronic pancreatitis management. https://pubmed.ncbi.nlm.nih.gov/26387697/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge