Osteochondral Fracture of the Talus: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Osteochondral fractures of the talus are relatively uncommon but clinically significant injuries involving damage to the articular cartilage and underlying subchondral bone. These lesions are most often associated with ankle trauma, particularly inversion injuries, and can lead to chronic pain, instability, and early osteoarthritis if not appropriately managed.
We report the case of a 28-year-old male who presented with persistent ankle pain and swelling following a sports-related injury. Imaging studies, including MRI, revealed an osteochondral fracture of the talar dome. The patient was treated with arthroscopic debridement and microfracture, followed by structured rehabilitation, resulting in favorable functional recovery.
This case highlights the importance of early recognition, appropriate imaging, and individualized management strategies in optimizing outcomes for osteochondral lesions of the talus.
Introduction
Osteochondral fractures of the talus, often referred to as osteochondral lesions of the talus (OLT), involve injury to both the cartilage and the underlying subchondral bone of the talar dome. These injuries are frequently overlooked in the acute setting, particularly when initial radiographs appear normal.
The talus plays a critical role in ankle biomechanics, transmitting forces between the leg and foot. Due to its limited vascular supply and high load-bearing function, injuries to the talus can have significant long-term consequences.
Osteochondral lesions are most commonly caused by trauma, particularly ankle sprains involving inversion or dorsiflexion. Medial lesions are typically deeper and associated with inversion and plantarflexion injuries, whereas lateral lesions tend to be more superficial and result from inversion and dorsiflexion mechanisms.
Risk factors include:
- Acute ankle trauma (sports injuries, falls)
- Recurrent ankle sprains
- High-impact athletic activities
- Delayed or missed diagnosis of ankle injuries
Clinically, patients may present with persistent ankle pain, swelling, stiffness, and mechanical symptoms such as locking or catching.
Case Report
Patient History
A 28-year-old male presented to the orthopedic outpatient department with complaints of:
- Persistent pain in the right ankle for 3 months
- Swelling aggravated by activity
- Difficulty in weight-bearing and running
- Occasional locking sensation in the ankle joint
The patient reported a history of a twisting injury to the ankle while playing football 3 months prior. He was initially managed conservatively with rest and analgesics, but symptoms persisted.
There was no history of previous ankle injuries, systemic illness, or inflammatory joint disease.
Clinical Examination
On general examination:
- Patient was afebrile
- Vital signs were stable
- No systemic abnormalities were noted
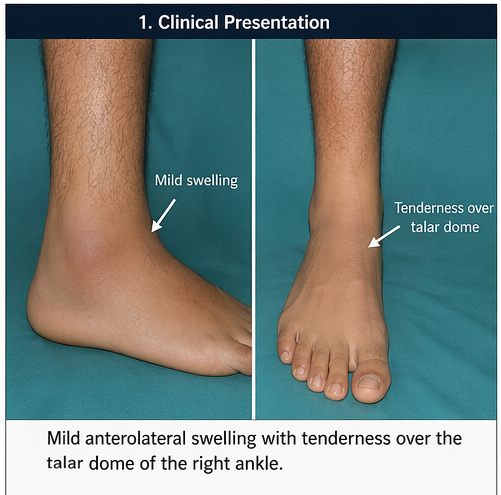
Local examination of the right ankle revealed:
- Mild swelling over the anterolateral aspect
- Tenderness over the talar dome region
- Pain on dorsiflexion and inversion
- Reduced range of motion compared to the contralateral ankle
- No gross instability on ligament testing
There were no signs of neurovascular compromise.
Clinical Evaluation
Differential Diagnosis
Based on clinical presentation, the following conditions were considered:
- Osteochondral fracture of the talus
- Chronic ankle sprain
- Synovitis of the ankle joint
- Talar dome contusion
- Early osteoarthritis
Persistent symptoms following an ankle injury raised suspicion for an osteochondral lesion.
Investigations
Radiological Findings
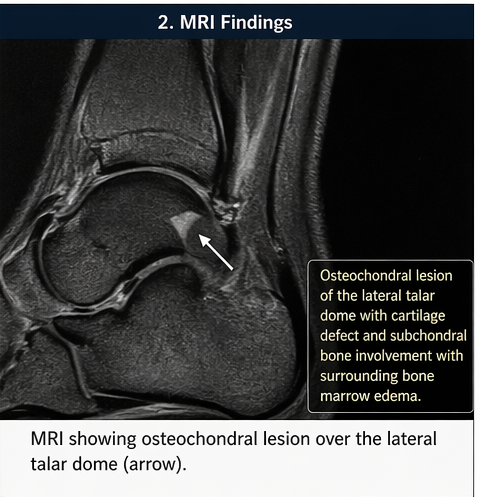
Plain Radiography:
- Initial X-rays were inconclusive, showing no obvious fracture
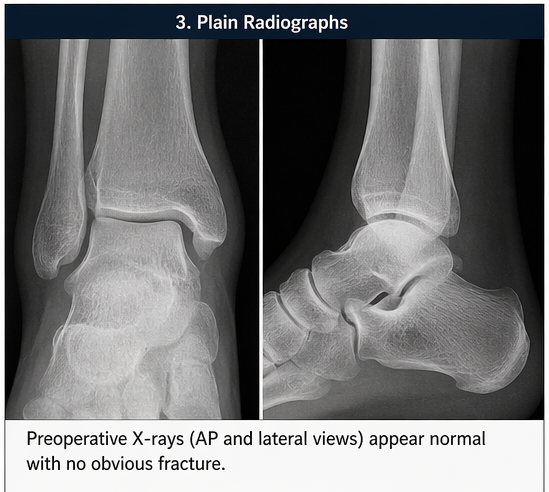
Magnetic Resonance Imaging (MRI):
- Revealed an osteochondral lesion over the lateral talar dome
- Evidence of cartilage defect with subchondral bone involvement
- Bone marrow edema surrounding the lesion
- No loose bodies identified
MRI played a crucial role in confirming the diagnosis and assessing lesion stability.
Diagnosis
Based on clinical findings and MRI imaging, a diagnosis of osteochondral fracture of the lateral talar dome was established.
Management and Outcome
Management Strategy
The treatment approach was individualized based on:
- Size and location of the lesion
- Symptom duration
- Functional impairment
Given the persistent symptoms and imaging findings, surgical intervention was planned.
Surgical Management
The patient underwent ankle arthroscopy, which revealed:
- A focal osteochondral defect over the lateral talar dome
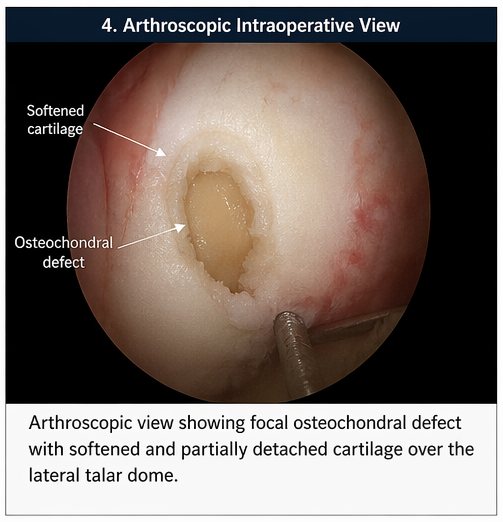
- Softened cartilage with partial detachment
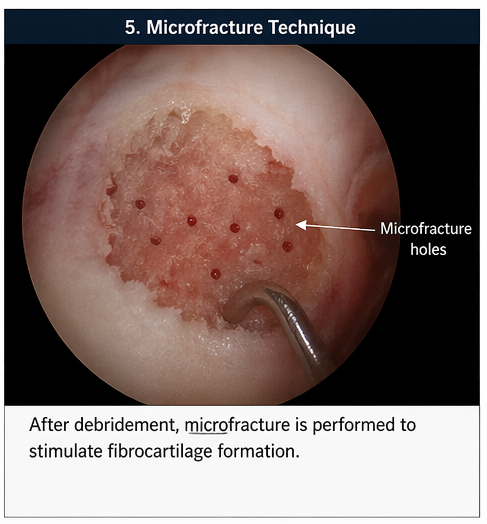
Procedures performed:
- Arthroscopic debridement of unstable cartilage
- Microfracture technique to stimulate fibrocartilage formation
The procedure was uneventful.
Postoperative Care
Postoperative management included:
- Non-weight-bearing for 4 weeks
- Gradual progression to partial and then full weight-bearing
- Physiotherapy focusing on:
- Range of motion exercises
- Strengthening of peri-ankle muscles
- Proprioceptive training
Follow-Up and Outcome
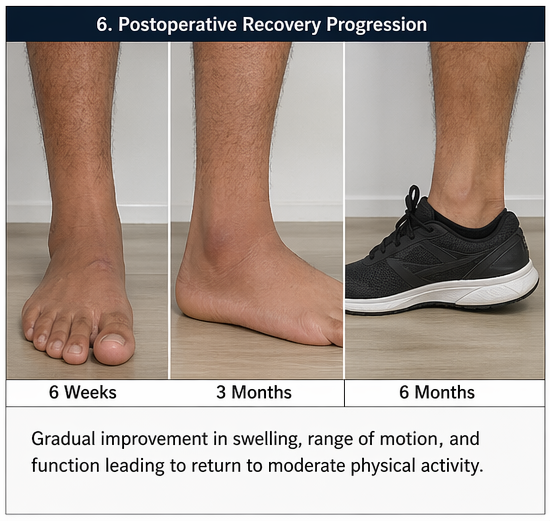
At 6 weeks:
- Reduction in pain
- Improved range of motion
At 3 months:
- Significant functional improvement
- Ability to bear weight without discomfort
- No mechanical symptoms
At 6 months:
- Return to moderate physical activity
- No recurrence of swelling or locking
- Improved ankle stability
The patient demonstrated excellent compliance with rehabilitation and achieved a favorable outcome.
Discussion
Pathophysiology
Osteochondral fractures of the talus occur due to shear and compressive forces acting on the articular surface during trauma. The injury results in:
- Disruption of cartilage integrity
- Damage to subchondral bone
- Potential formation of loose fragments
The talus has a relatively poor blood supply, which limits healing potential and increases the risk of chronic lesions.
Classification
Osteochondral lesions are commonly classified based on imaging findings:
- Stable vs unstable lesions
- Displaced vs non-displaced fragments
MRI-based classifications help guide treatment decisions.
Diagnostic Challenges
Diagnosis can be challenging due to:
- Normal initial radiographs
- Overlap with simple ankle sprains
- Delayed presentation of symptoms
MRI is the gold standard for detecting early lesions and assessing cartilage integrity.
Treatment Considerations
Management depends on lesion characteristics and symptom severity.
Conservative Management:
- Indicated for small, stable lesions
- Includes rest, immobilization, and physiotherapy
Surgical Management:
- Indicated for:
- Persistent symptoms
- Large or unstable lesions
- Failure of conservative therapy
Surgical options include:
- Arthroscopic debridement
- Microfracture
- Osteochondral autograft transplantation
- Autologous chondrocyte implantation
Complications
If untreated or inadequately managed, osteochondral fractures may lead to:
- Chronic ankle pain
- Joint instability
- Osteoarthritis
- Reduced functional capacity
Post-surgical complications may include:
- Incomplete healing
- Fibrocartilage degeneration
- Recurrence of symptoms
Prognosis
The prognosis depends on:
- Size and location of the lesion
- Timeliness of diagnosis
- Type of treatment
- Patient adherence to rehabilitation
Early intervention generally leads to better outcomes. Microfracture techniques are effective for small to medium-sized lesions, though long-term durability may vary.
Conclusion
Osteochondral fractures of the talus are important yet often underdiagnosed injuries following ankle trauma. This case emphasizes the need for a high index of suspicion in patients with persistent ankle symptoms despite initial conservative management.
MRI plays a critical role in diagnosis, while arthroscopic management offers effective treatment for symptomatic lesions. A multidisciplinary approach involving orthopedic surgeons and physiotherapists is essential for optimal recovery.
Timely diagnosis and appropriate intervention can significantly improve functional outcomes and prevent long-term complications such as osteoarthritis. Increased awareness among clinicians is key to ensuring early detection and effective management of this condition.
References
- Berndt, A. L., & Harty, M. (1959). Transchondral fractures (osteochondritis dissecans) of the talus. The Journal of Bone and Joint Surgery. American Volume. https://pubmed.ncbi.nlm.nih.gov/13849029/
- Verhagen, R. A. W., Struijs, P. A. A., Bossuyt, P. M. M., & van Dijk, C. N. (2003). Systematic review of treatment strategies for osteochondral defects of the talar dome. Foot and Ankle Clinics, 8(2), 233–242. https://pubmed.ncbi.nlm.nih.gov/12911238/
- Tol, J. L., Struijs, P. A. A., Bossuyt, P. M. M., Verhagen, R. A. W., & van Dijk, C. N. (2000). Treatment strategies in osteochondral defects of the talar dome: A systematic review. Foot & Ankle International, 21(2), 119–126. https://pubmed.ncbi.nlm.nih.gov/10694023/
- Schuman, L., Struijs, P. A. A., & van Dijk, C. N. (2002). Arthroscopic treatment for osteochondral defects of the talus. Results at follow-up at 2 to 11 years. The Journal of Bone and Joint Surgery. British Volume, 84(3), 364–368. https://pubmed.ncbi.nlm.nih.gov/12002494/
- Easley, M. E., & Scranton, P. E. (2003). Osteochondral lesions of the talus. The Journal of the American Academy of Orthopaedic Surgeons, 11(6), 405–414. https://pubmed.ncbi.nlm.nih.gov/14601379/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge