Tuberculous Meningitis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Tuberculous meningitis (TBM) is the most severe form of extrapulmonary tuberculosis, associated with high mortality and long-term neurological sequelae if diagnosis and treatment are delayed. It results from hematogenous dissemination of Mycobacterium tuberculosis to the meninges, leading to granulomatous inflammation, vasculitis, and raised intracranial pressure. Clinical manifestations are often subacute and include fever, headache, altered sensorium, vomiting, cranial nerve palsies, and focal neurological deficits. Early recognition is challenging due to nonspecific symptoms and limited sensitivity of conventional diagnostic tests. Prompt initiation of antitubercular therapy with adjunctive corticosteroids is essential to improve survival and neurological outcomes. We report a case of tuberculous meningitis in an elderly male presenting with subacute fever, progressive headache, and altered mental status. The case highlights clinical presentation, diagnostic evaluation including cerebrospinal fluid (CSF) analysis and neuroimaging, immediate management with antitubercular therapy and corticosteroids, and short-term outcomes. Early diagnosis, timely treatment, and close neurological monitoring remain crucial to reduce morbidity and prevent long-term disability.
Introduction
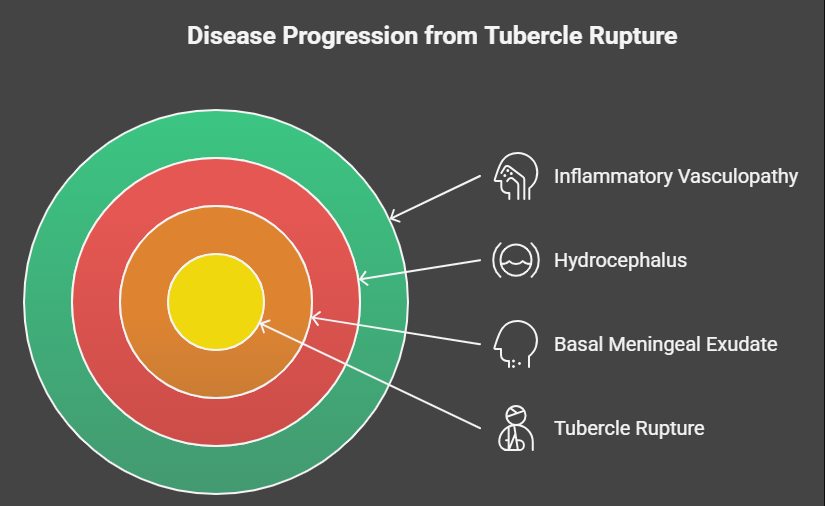
Tuberculous meningitis represents a medical emergency and accounts for a substantial proportion of morbidity and mortality associated with tuberculosis, particularly in low- and middle-income countries. The disease arises from rupture of a subependymal or subpial tubercle into the subarachnoid space, resulting in a basal meningeal exudate, hydrocephalus, and inflammatory vasculopathy.
Risk factors include advanced age, malnutrition, diabetes mellitus, chronic kidney disease, immunosuppression, and poor socioeconomic conditions.
Clinical presentation is often insidious, with prodromal symptoms preceding overt neurological involvement. Delay in diagnosis is common and strongly associated with poor outcomes, including persistent neurological deficits, stroke, and death. Diagnosis relies on a combination of clinical suspicion, CSF analysis, microbiological testing, and neuroimaging. Management requires prolonged multidrug antitubercular therapy, adjunctive corticosteroids, management of raised intracranial pressure, and supportive neurocritical care. Early recognition and prompt treatment are essential determinants of prognosis.
Case Report
Patient History
A 62-year-old male presented to the emergency department with low-grade fever, progressive headache, and intermittent vomiting for 3 weeks, followed by altered sensorium and unsteady gait for 2 days. He reported generalized weakness and reduced appetite but denied seizures or recent head trauma. There was no history of cough, hemoptysis, or known tuberculosis contact. The patient had poorly controlled type 2 diabetes mellitus for 10 years and had lost approximately 5 kg over the preceding 2 months. There was no history of HIV infection or chronic steroid use.
Clinical Examination
On admission, the patient was drowsy but arousable. Vital signs: temperature 38.4°C, blood pressure 130/80 mmHg, heart rate 98 bpm, respiratory rate 20/min, oxygen saturation 96% on room air.

Neurological examination revealed neck stiffness and positive Kernig’s sign. Cranial nerve examination showed mild left sixth nerve palsy. Motor examination revealed mild right-sided weakness (power 4/5) with brisk reflexes. Fundoscopy demonstrated early papilledema. Cardiovascular, respiratory, and abdominal examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
- Tuberculous meningitis
- Acute bacterial meningitis
- Viral meningoencephalitis
- Fungal meningitis
- Subacute meningoencephalitis secondary to malignancy
Investigations
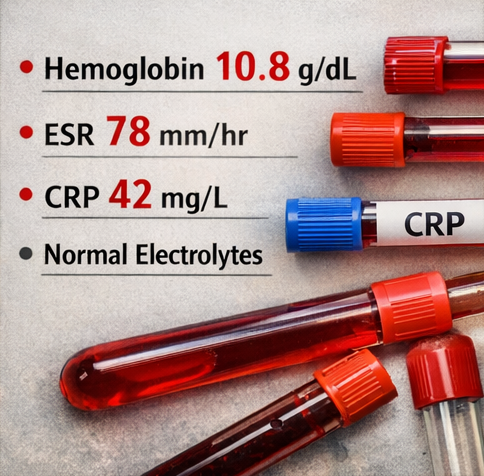
- Blood tests: Mild anemia (Hb 10.8 g/dL), elevated ESR (78 mm/hr), C-reactive protein 42 mg/L, normal electrolytes
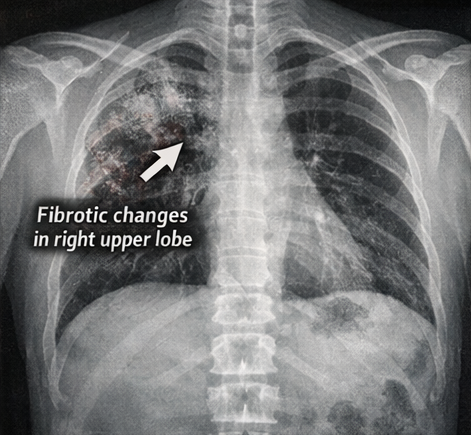
- Chest X-ray: Patchy fibrotic changes in the right upper lobe suggestive of old healed tuberculosis
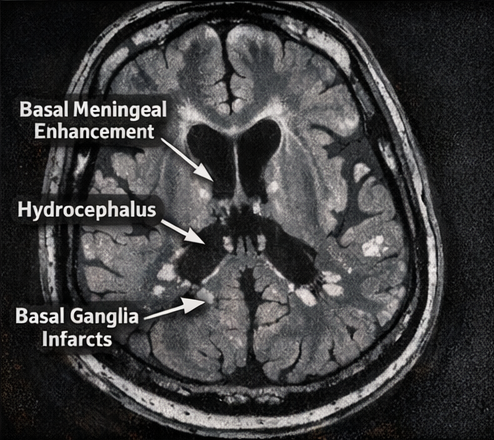
- Neuroimaging (MRI brain with contrast): Basal meningeal enhancement, communicating hydrocephalus, and multiple small infarcts in the basal ganglia consistent with tuberculous vasculitis
- Lumbar puncture (CSF analysis):
- Opening pressure: elevated
- Appearance: clear
- Cells: 180 cells/mm³ (lymphocytic predominance)
- Protein: 220 mg/dL (elevated)
- Glucose: 32 mg/dL (with corresponding blood glucose 120 mg/dL)
- CSF ADA: elevated
- Microbiology: Acid-fast bacilli smear negative; nucleic acid amplification test positive for Mycobacterium tuberculosis; rifampicin resistance not detected
- HIV test: Negative
These findings were consistent with tuberculous meningitis with associated hydrocephalus and vasculitic infarcts.
Management and Outcome
Management Strategy
The patient was managed in a high-dependency neurological unit. Immediate treatment included:
- Antitubercular therapy (ATT):
- Intensive phase: Isoniazid, rifampicin, pyrazinamide, and ethambutol
- Adjunctive corticosteroids:
- Dexamethasone intravenously, followed by a planned taper over 6–8 weeks
- Management of raised intracranial pressure:
- Head elevation, osmotherapy as needed, careful fluid balance
- Supportive care:
- Antiemetics, analgesia, glycemic control with insulin
- Monitoring:
- Regular neurological assessments, visual acuity monitoring, liver function tests
Neurosurgical consultation was obtained for hydrocephalus. As the patient remained clinically stable with improving consciousness, conservative management was continued without immediate CSF diversion.
Follow-Up and Outcome
Over the first week of therapy, the patient showed gradual improvement in alertness and reduction in headache and vomiting. By day 10, the sixth nerve palsy had partially improved, and right-sided weakness diminished. Repeat imaging after 3 weeks showed stable ventricular size and no new infarcts. The patient was discharged after 4 weeks on continuation-phase ATT with oral steroids on taper.
At 2-month follow-up, he was ambulatory with minimal residual gait unsteadiness and had no further episodes of altered sensorium. Neurocognitive function improved, and adherence to prolonged ATT was reinforced. Long-term follow-up was planned for 12 months of therapy with periodic neurological and imaging assessments.
Discussion
Tuberculous meningitis remains a devastating neurological emergency with high rates of mortality and neurological disability. The subacute presentation and low sensitivity of conventional microbiological tests often delay diagnosis. CSF typically shows lymphocytic pleocytosis, elevated protein, and low glucose; however, microbiological confirmation may require nucleic acid amplification tests or culture, which can take time. Neuroimaging commonly demonstrates basal meningeal enhancement, hydrocephalus, and infarcts due to vasculitis, all of which correlate with worse outcomes.
Management requires prolonged multidrug ATT due to poor CNS penetration of some agents and high bacillary burden within the meninges. Adjunctive corticosteroids reduce mortality and the risk of disabling neurological sequelae by attenuating inflammatory damage and cerebral edema. Early recognition of complications such as hydrocephalus, vasculitic strokes, hyponatremia, and cranial neuropathies is essential. Multidisciplinary care involving neurology, infectious diseases, neurosurgery, and rehabilitation optimizes outcomes. Delayed therapy is strongly associated with persistent cognitive deficits, motor disability, and death, underscoring the need for high clinical suspicion in endemic regions.
Conclusion
Tuberculous meningitis is a life-threatening form of extrapulmonary tuberculosis requiring urgent diagnosis and aggressive management. Subacute meningeal symptoms with constitutional features in high-risk individuals should prompt immediate evaluation for TBM. Early initiation of antitubercular therapy with adjunctive corticosteroids, management of raised intracranial pressure, and close neurological monitoring can significantly improve survival and functional outcomes. Long-term follow-up and adherence to prolonged therapy are essential to prevent relapse and minimize long-term neurological sequelae.
References
- Thwaites GE, et al. Tuberculous meningitis. Lancet. 2013;381(9871):1249–1258.
- Marais S, et al. Tuberculous meningitis: A uniform case definition for use in clinical research. Lancet Infect Dis. 2010;10(11):803–812.
- Prasad K, Singh MB. Corticosteroids for managing tuberculous meningitis. Cochrane Database Syst Rev. 2016;4:CD002244.
- Rock RB, et al. Central nervous system tuberculosis: Pathogenesis and clinical aspects. Clin Microbiol Rev. 2008;21(2):243–261.
- Wilkinson RJ, et al. Tuberculous meningitis. Nat Rev Neurol. 2017;13(10):581–598.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Potential targets for treating the most common type of liver cancer in children have been identified by a collaborative study.
2.
Study identifies new approach to protect the brain during radiation therapy
3.
While most cancer screenings won't prolong lives, there are still good reasons to continue screening.
4.
Chemo-Free Quadruplet Shows Promise as DLBCL's First Therapy.
5.
Radiation therapy for patients with breast cancer
1.
Radiation in Oncology: Advances, Applications, and Accessibility
2.
The Next Generation of Precision: How Multi-Specific Antibodies are Redefining Oncology's Future - A 2025 Review
3.
Cracking Oncology Drug Resistance: New Strategies to Overcome Challenges in Modern Cancer Therapy
4.
Unlocking the Secrets of Neutrophils: Exploring Their Role in Immune Defense
5.
Precision Oncology: Personalized Medicine Shaping the Future of Cancer Care
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib Takes Center Stage in Managing Renal Cell Carcinoma - Part II
2.
Recent Data Analysis for First-Line Treatment of ALK+ NSCLC
3.
Navigating the Complexities of Ph Negative ALL - Part XIII
4.
Navigating the Complexities of Ph Negative ALL - Part IV
5.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part VIII

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge