Oral Carcinoma: Clinical Evaluation, Multidisciplinary Management, and Outcome - A Case Report
OthersPage Navigation
Abstract
Oral carcinoma is a major public health concern worldwide, particularly in developing countries where tobacco use, betel nut chewing, and alcohol consumption are prevalent. Squamous cell carcinoma accounts for the majority of oral malignancies and is often diagnosed at an advanced stage due to delayed presentation. Clinical manifestations range from non-healing oral ulcers and mucosal lesions to pain, dysphagia, and regional lymphadenopathy. Accurate diagnosis relies on thorough clinical examination, histopathological confirmation, and appropriate imaging for staging. Management requires a multidisciplinary approach involving surgical oncology, radiation oncology, medical oncology, pathology, and rehabilitation services. We report a case of oral squamous cell carcinoma of the buccal mucosa in a middle-aged male presenting with a non-healing ulcer and cervical lymphadenopathy. A coordinated multidisciplinary treatment strategy resulted in effective tumor control and satisfactory functional outcomes. This case highlights the importance of early recognition, comprehensive staging, and integrated care in improving prognosis and quality of life in patients with oral carcinoma.
Introduction
Oral carcinoma represents a significant proportion of head and neck cancers and remains a leading cause of cancer-related morbidity and mortality globally [1]. The disease burden is particularly high in South and Southeast Asia, largely attributable to widespread use of smokeless tobacco, betel quid, areca nut, and alcohol. Oral squamous cell carcinoma (OSCC) constitutes approximately 90% of all oral malignancies.
The pathogenesis of oral carcinoma is multifactorial, involving chronic mucosal irritation, exposure to carcinogens, viral infections such as human papillomavirus (HPV), and genetic susceptibility [2]. Common sites include the buccal mucosa, tongue, floor of the mouth, gingiva, and hard palate. Early-stage lesions may present as leukoplakia, erythroplakia, or small ulcers, whereas advanced disease is associated with pain, bleeding, trismus, dysphagia, and cervical lymph node metastasis.
Early diagnosis and accurate staging are crucial determinants of prognosis. Advances in imaging, surgical techniques, reconstructive surgery, and adjuvant therapies have significantly improved survival and functional outcomes. This case report describes the clinical presentation, diagnostic workup, and multidisciplinary management of a patient with oral squamous cell carcinoma.
Case Report
Patient History
A 52-year-old male presented to the head and neck oncology clinic with a non-healing ulcer over the right buccal mucosa for three months. The lesion was initially painless but gradually increased in size and was associated with mild pain and occasional bleeding. Over the past four weeks, the patient noticed difficulty in chewing and a swelling on the right side of the neck.
The patient had a 25-year history of smokeless tobacco chewing and occasional alcohol consumption. There was no history of prior oral lesions, radiation exposure, or significant systemic illness. Family history was non-contributory.
Clinical Examination
On general examination, the patient was moderately built and nourished. Vital signs were stable. Oral cavity examination revealed a 3 × 2 cm irregular ulceroproliferative lesion on the right buccal mucosa, with indurated margins and a granular base. The lesion was tender on palpation and bled on contact. There was reduced mobility of the adjacent mucosa.
Neck examination revealed a single, firm, non-tender, mobile right submandibular lymph node measuring approximately 2 cm in diameter. No other cervical lymphadenopathy was noted. Mouth opening was mildly restricted, and cranial nerve examination was normal.
Investigations
Histopathology
An incisional biopsy of the oral lesion was performed. Histopathological examination revealed invasive well-differentiated squamous cell carcinoma, characterized by malignant squamous cells forming keratin pearls and infiltrating the underlying stroma.

Imaging Studies
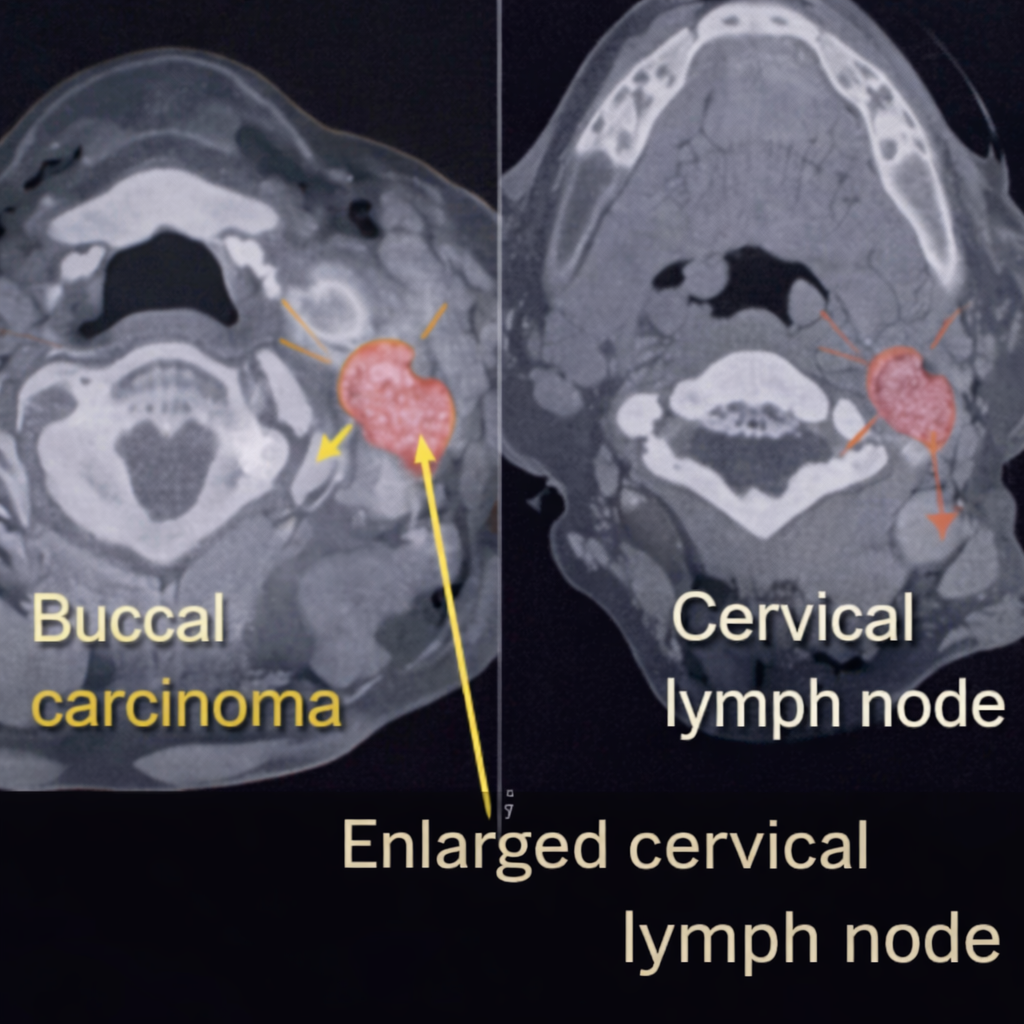
Contrast-enhanced computed tomography (CT) scan of the face and neck demonstrated a localized soft tissue mass involving the right buccal mucosa without mandibular invasion. A single enlarged right level Ib lymph node was noted, with preserved fatty hilum and no evidence of extranodal extension. Chest imaging showed no distant metastasis.
Diagnosis
Based on clinical, histopathological, and radiological findings, a diagnosis of oral squamous cell carcinoma of the right buccal mucosa, clinical stage T2N1M0, was established.
Management and Outcome
Multidisciplinary Approach
The case was discussed in a multidisciplinary tumor board comprising head and neck surgeons, medical oncologists, radiation oncologists, radiologists, pathologists, anesthesiologists, and speech and swallowing therapists. Considering the stage of disease and nodal involvement, primary surgical management followed by adjuvant therapy was planned.

Surgical Management
The patient underwent wide local excision of the buccal mucosal lesion with adequate oncologic margins, along with right selective neck dissection (levels I–III). Reconstruction of the mucosal defect was achieved using a local advancement flap to preserve oral function.
Intraoperatively, the tumor was confined to the buccal mucosa without bone involvement. Critical neurovascular structures were preserved, and hemostasis was secured. The postoperative course was uneventful.
Histopathological Findings
The resected specimen confirmed well-differentiated squamous cell carcinoma with clear surgical margins. One of the dissected cervical lymph nodes showed metastatic involvement without extracapsular spread. Perineural and lymphovascular invasion were absent.
Adjuvant Therapy and Follow-Up
Based on final histopathology, the patient received adjuvant external beam radiotherapy to the primary site and neck. Nutritional support, oral hygiene measures, and speech therapy were initiated during recovery.
At six-month follow-up, the patient remained disease-free, with satisfactory oral intake and speech. There was no evidence of local recurrence or distant metastasis. The patient reported significant improvement in quality of life and had discontinued tobacco use.

Discussion
Oral squamous cell carcinoma is a preventable malignancy strongly associated with modifiable risk factors. Despite advances in therapy, delayed presentation remains a major challenge, contributing to poor outcomes [3].
Comprehensive evaluation, including biopsy and imaging, is essential for accurate staging and treatment planning. Surgical resection remains the cornerstone of management for resectable disease, with adjuvant radiotherapy or chemoradiotherapy indicated in selected cases based on pathological risk factors [4].
Multidisciplinary management is critical to optimize oncologic control while preserving speech, swallowing, and aesthetics. Early rehabilitation and long-term surveillance play an important role in functional recovery and early detection of recurrence [5].
Conclusion
Oral carcinoma requires a high index of clinical suspicion and prompt diagnostic evaluation, particularly in high-risk individuals. This case demonstrates that early-stage oral squamous cell carcinoma, when managed with a structured multidisciplinary approach, can achieve excellent oncologic and functional outcomes. Public awareness, risk factor modification, early diagnosis, and coordinated care remain key strategies in reducing the burden of oral cancer.
References
- Warnakulasuriya S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009;45(4–5):309–316.
- Neville BW, Day TA. Oral cancer and precancerous lesions. CA Cancer J Clin. 2002;52(4):195–215.
- Gupta B, Johnson NW. Systematic review and meta-analysis of association of smokeless tobacco and oral cancer. PLoS One. 2014;9(2):e88748.
- National Comprehensive Cancer Network (NCCN). Head and Neck Cancers Guidelines. Version 2023.
- Shah JP, Gil Z. Current concepts in management of oral cancer. Surg Oncol Clin N Am. 2015;24(3):491–510.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Researchers find distinct cell receptors with the potential for new treatments.
2.
Breast cancer patients' arms swell less after an effective lymph node transfer.
3.
Telehealth in the pandemic era resulted in fewer therapy interruptions.
4.
Too Many Chest CTs for Incidental Lung Nodules?
5.
Global warming could be driving up women's cancer risk, find researchers
1.
The New Frontier of Cancer Survivorship: Navigating the Long-Term Effects of Immunotherapy and Targeted Therapies
2.
Deterministic Reprogramming of Neutrophils within Tumors: A New Frontier in Cancer Research
3.
Neuroendocrine Tumors: Case Study on Diagnosis, Treatment Strategies & Patient Management
4.
Ticagrelor Monotherapy vs. Ticagrelor + Aspirin in ACS Post-PCI: ULTIMATE-DAPT Trial
5.
Transfusing the Future: Exploring the Possibilities of Blood Transfusions
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Current Scenario of Blood Cancer- A Conclusion on Genomic Testing & Advancement in Diagnosis and Treatment
2.
Navigating the Brain Barrier: The CNS Challenge in ALK+ NSCLC
3.
Thromboprophylaxis In Medical Settings
4.
Treatment Paradigm for Patients with R/R Adult B-cell ALL- Expert Discussions
5.
Current Scenario of Blood Cancer- Genomic Testing & Advancement in Diagnosis and Treatment

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge