Tuberculosis: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Tuberculosis (TB) remains a major global public health concern, particularly in low- and middle-income countries, despite the availability of effective diagnostic tools and curative therapy. Caused by Mycobacterium tuberculosis, TB most commonly affects the lungs but can involve virtually any organ system. Clinical presentation is often insidious, leading to delayed diagnosis and increased risk of transmission and complications. Pulmonary TB typically presents with chronic cough, fever, weight loss, and hemoptysis, while extrapulmonary manifestations vary depending on the site of involvement. Diagnosis relies on a combination of clinical suspicion, microbiological confirmation, radiological findings, and molecular testing. Early initiation of standardized anti-tubercular therapy is essential to achieve cure, prevent relapse, and limit disease spread. This case report describes an adult patient diagnosed with pulmonary tuberculosis, highlighting the clinical features, diagnostic workup, treatment approach, and short-term outcomes, while emphasizing the importance of early recognition and adherence to therapy.
Introduction
Tuberculosis is a chronic infectious disease caused by Mycobacterium tuberculosis, transmitted primarily through airborne droplets. Despite significant advances in diagnostics and therapeutics, TB remains one of the leading causes of death from infectious diseases worldwide. The disease burden is disproportionately high in developing regions, where factors such as overcrowding, malnutrition, delayed healthcare access, and comorbidities contribute to sustained transmission.
Pulmonary TB accounts for the majority of cases and represents the primary source of disease spread. The disease often follows a slow and progressive course, with nonspecific symptoms that may mimic other respiratory illnesses, leading to diagnostic delays. Untreated TB can result in extensive lung destruction, respiratory failure, systemic complications, and death.
Early diagnosis, prompt initiation of treatment, and strict adherence to standardized treatment regimens are critical for disease control. This case report presents a typical presentation of pulmonary tuberculosis in an immunocompetent adult, focusing on clinical evaluation, diagnostic strategies, management, and outcomes.
Case Report
Patient History
A 45-year-old male presented to the outpatient respiratory clinic with complaints of persistent cough for six weeks, intermittent low-grade fever, night sweats, and unintentional weight loss of approximately 6 kilograms over two months. The cough was initially dry but had become productive with scant mucoid sputum. There was no history of hemoptysis at presentation.

The patient worked as a factory laborer and reported living in a crowded urban setting. He denied any previous history of tuberculosis, chronic lung disease, diabetes mellitus, or immunosuppressive conditions. There was no known contact with a diagnosed TB patient. He was a non-smoker and did not consume alcohol regularly.
Clinical Examination
On general examination, the patient appeared thin and fatigued. Vital signs revealed a temperature of 37.9°C, heart rate of 92 beats per minute, blood pressure of 122/76 mmHg, and oxygen saturation of 97% on room air.
Respiratory system examination revealed reduced chest expansion on the right side and coarse crackles over the right upper lung field. No wheezing was noted. There was no peripheral lymphadenopathy, clubbing, or pedal edema. Cardiovascular and abdominal examinations were unremarkable.
Clinical Evaluation
Differential Diagnosis
Based on the clinical presentation, the following differential diagnoses were considered:
• Pulmonary tuberculosis
• Community-acquired pneumonia
• Chronic bronchitis
• Lung malignancy
• Fungal pulmonary infection
The chronicity of symptoms, constitutional features, and occupational exposure raised a high clinical suspicion for pulmonary tuberculosis.
Investigations
Laboratory Tests:
• Complete blood count: Mild normocytic anemia
• Erythrocyte sedimentation rate: Elevated
• C-reactive protein: Mildly elevated
• Liver and renal function tests: Within normal limits
• HIV serology: Negative
Microbiological Evaluation:
• Sputum smear microscopy: Positive for acid-fast bacilli
• Cartridge-based nucleic acid amplification test (CBNAAT): Detected Mycobacterium tuberculosis with no rifampicin resistance
Radiological Evaluation:
• Chest X-ray: Right upper lobe infiltrates with patchy consolidation and cavitary lesions
• High-resolution computed tomography (HRCT) chest: Confirmed cavitary disease in the right upper lobe with surrounding nodular opacities and tree-in-bud appearance
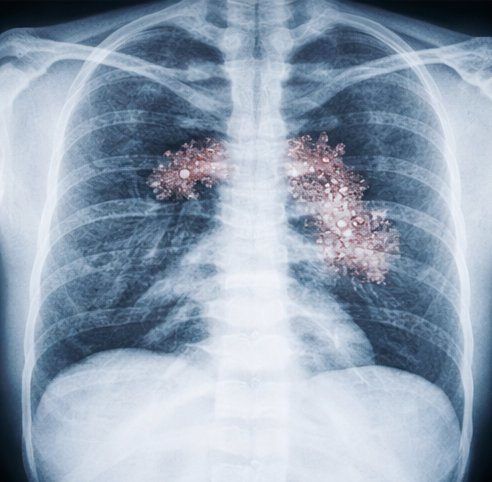
These findings confirmed the diagnosis of drug-sensitive pulmonary tuberculosis.
Management and Outcome
Initial Management
The patient was counseled regarding the diagnosis, disease transmission, treatment duration, and importance of adherence. He was registered under the national tuberculosis control program and initiated on standard first-line anti-tubercular therapy.
Anti-tubercular regimen (Intensive Phase):
• Isoniazid
• Rifampicin
• Pyrazinamide
• Ethambutol
The medications were administered as fixed-dose combinations under directly observed treatment. Pyridoxine supplementation was provided to prevent isoniazid-induced neuropathy.

Supportive Care
• Nutritional counseling with emphasis on high-protein, calorie-dense diet
• Symptomatic treatment for fever and cough
• Patient education on cough hygiene and infection control measures
Baseline vision assessment and liver function tests were documented prior to therapy initiation.
Follow-Up and Outcome
At the end of the intensive phase (two months), the patient reported significant symptomatic improvement, including resolution of fever and night sweats, improved appetite, and weight gain of 3 kilograms. Cough frequency had markedly reduced.

Repeat sputum smear examination was negative for acid-fast bacilli. Liver function tests remained within normal limits. The patient was transitioned to the continuation phase with isoniazid and rifampicin for an additional four months.
At completion of six months of therapy, the patient was asymptomatic, had regained baseline body weight, and demonstrated radiological improvement on chest imaging. He was declared cured based on clinical, microbiological, and radiological criteria.
Discussion
Tuberculosis remains a disease of significant clinical and public health importance. This case illustrates a classic presentation of pulmonary TB in an immunocompetent adult, emphasizing the importance of maintaining a high index of suspicion in patients presenting with chronic respiratory symptoms and constitutional features.
The insidious onset of symptoms often leads to delayed healthcare seeking, increasing the risk of disease transmission and lung damage. Microbiological confirmation remains the cornerstone of diagnosis, with molecular tests enabling rapid detection and drug-resistance assessment.
Radiological findings, particularly upper lobe cavitation, are characteristic of pulmonary TB and correlate with higher bacillary load and infectivity. Early initiation of standardized therapy leads to high cure rates and prevents long-term complications.
Adherence to therapy is critical, as incomplete or irregular treatment can result in relapse or development of drug-resistant TB. Patient education, nutritional support, and regular follow-up are integral components of successful management.
This case highlights the effectiveness of current treatment protocols when applied promptly and emphasizes the importance of early diagnosis and structured follow-up in achieving favorable outcomes.
Conclusion
Tuberculosis is a potentially curable disease when diagnosed early and treated appropriately. Chronic cough, weight loss, and fever should prompt evaluation for TB, particularly in high-risk populations. A combination of clinical assessment, microbiological testing, and imaging facilitates accurate diagnosis. Standardized anti-tubercular therapy, along with patient education and adherence monitoring, leads to excellent outcomes. Strengthening early detection and treatment strategies remains essential for reducing TB-related morbidity and transmission.
References
- World Health Organization. (2023). Global tuberculosis report. https://www.who.int/teams/global-tuberculosis-programme/tb-reports
- Pai, M., Behr, M. A., Dowdy, D., et al. (2016). Tuberculosis. Nature Reviews Disease Primers, 2, 16076 https://pubmed.ncbi.nlm.nih.gov/27784885/
- Lewinsohn, D. M., Leonard, M. K., LoBue, P. A., et al. (2017). Official American Thoracic Society guidelines: Diagnosis of tuberculosis in adults and children. Clinical Infectious Diseases, 64(2), 111–115 https://pubmed.ncbi.nlm.nih.gov/28052967/
- Sharma, S. K., & Mohan, A. (2013). Tuberculosis: From an incurable scourge to a curable disease. Journal of the Association of Physicians of India, 61(6), 403–407. https://pubmed.ncbi.nlm.nih.gov/24475532
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Sub-Q Ketamine is Safe and Very Effective for Severe Depression.
2.
Study indicates that exercise can help colon cancer survivors live as long as matched individuals
3.
Contradictory Results Are Found in Two Pembrolizumab Trials for Head and Neck Cancer.
4.
Can Concurrent Boost Safely Shorten Breast Cancer Radiation?
5.
Positive Trials; Malignancies Increasing in Younger Adults; Andre Braugher's Cancer Dx.
1.
Trends in Incidence, Care, and Surgery for Medullary Thyroid Cancer: A Review
2.
Antibody-Drug Conjugates in Oncology: Breakthroughs, Clinical Updates, and Pipeline Innovation
3.
Navigating the Stages of Thyroid Cancer: A Guide for Patients
4.
Polycythemia Vera: A Historical Perspective and Contemporary Management
5.
Glofitamab: A Breakthrough Therapy for Relapsed/Refractory Mantle Cell Lymphoma
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Pazopanib: A Game-Changer in Managing Advanced Renal Cell Carcinoma - Part IV
2.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VIII
3.
Evolving Space of First-Line Treatment for Urothelial Carcinoma- Case Discussion
4.
Key Takeaways from The CROWN Trial For ALK + NSCLC Patients with CNS Diseases
5.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part I

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge