Alopecia Areata: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Alopecia areata is a chronic, immune-mediated, non-scarring hair loss disorder characterized by sudden onset of patchy hair loss affecting the scalp and other hair-bearing areas. It results from autoimmune attack on anagen hair follicles, leading to localized or generalized alopecia. The disease spectrum ranges from limited patchy involvement to alopecia totalis and alopecia universalis. Although not life-threatening, alopecia areata significantly impacts psychosocial well-being and quality of life. Diagnosis is primarily clinical, supported by dermoscopy (trichoscopy) and, in selected cases, histopathological examination. Management depends on disease severity and may include topical, intralesional, systemic immunosuppressive therapies, and newer targeted agents such as Janus kinase (JAK) inhibitors. This case report describes a middle-aged female presenting with patchy scalp hair loss, highlighting clinical evaluation, diagnostic approach, therapeutic strategy, and outcomes.
Introduction
Alopecia areata is an organ-specific autoimmune disorder targeting hair follicles, particularly during the anagen phase. The condition affects approximately 1–2% of the global population over a lifetime and can occur at any age, with a peak incidence in young adults. Both genetic susceptibility and environmental triggers contribute to disease onset.
The pathogenesis involves loss of immune privilege of the hair follicle, mediated by autoreactive T lymphocytes and pro-inflammatory cytokines such as interferon-gamma. Associations with other autoimmune conditions—including thyroid disorders, vitiligo, type 1 diabetes mellitus, and atopic disease—are well documented.
Clinically, alopecia areata presents with well-circumscribed patches of non-scarring hair loss. Nail changes such as pitting may be present. The course is unpredictable, with spontaneous remission in some patients and chronic relapsing disease in others. Recent advances in targeted immunotherapy have expanded treatment options, particularly for extensive disease.
This report presents a case of localized alopecia areata, emphasizing diagnostic evaluation and therapeutic outcomes.
Case Report
Patient History
A 34-year-old female presented to the dermatology outpatient clinic with complaints of sudden onset hair loss over the scalp for three months. She reported noticing a small coin-sized bald patch over the occipital region, which gradually increased in size. Over the following weeks, two additional patches developed over the parietal scalp.
There was no associated itching, pain, scaling, or discharge. The patient denied recent febrile illness, significant stress, or new medication use. There was no history of traction hairstyles, chemical hair treatments, or cosmetic procedures.
Her medical history was notable for autoimmune hypothyroidism diagnosed five years earlier, controlled with levothyroxine. There was a family history of vitiligo in her mother. No prior episodes of similar hair loss were reported.
Clinical Examination
General examination was unremarkable. The patient appeared anxious regarding cosmetic concerns but was otherwise stable.
Scalp examination revealed three well-demarcated, smooth, round to oval patches of non-scarring alopecia measuring 2–4 cm in diameter. The overlying skin appeared normal without erythema, scaling, or atrophy. No scarring or follicular plugging was observed.
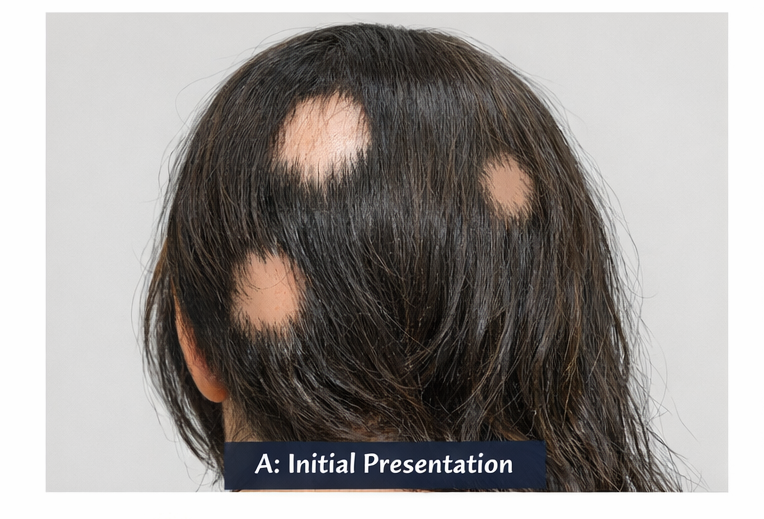
Exclamation mark hairs were visible at the margins of the patches. Gentle hair pull test was positive at the periphery of active lesions.
Eyebrows, eyelashes, and body hair were preserved. Nail examination revealed subtle pitting in several fingernails.
There was no lymphadenopathy or systemic abnormality.
Clinical Evaluation
Differential Diagnosis
Based on history and examination, the following differential diagnoses were considered:
• Alopecia areata
• Tinea capitis
• Trichotillomania
• Telogen effluvium
• Early scarring alopecia
The absence of scaling, inflammation, broken hairs of varying length, and scarring favored alopecia areata.
Investigations
Dermoscopy (Trichoscopy)
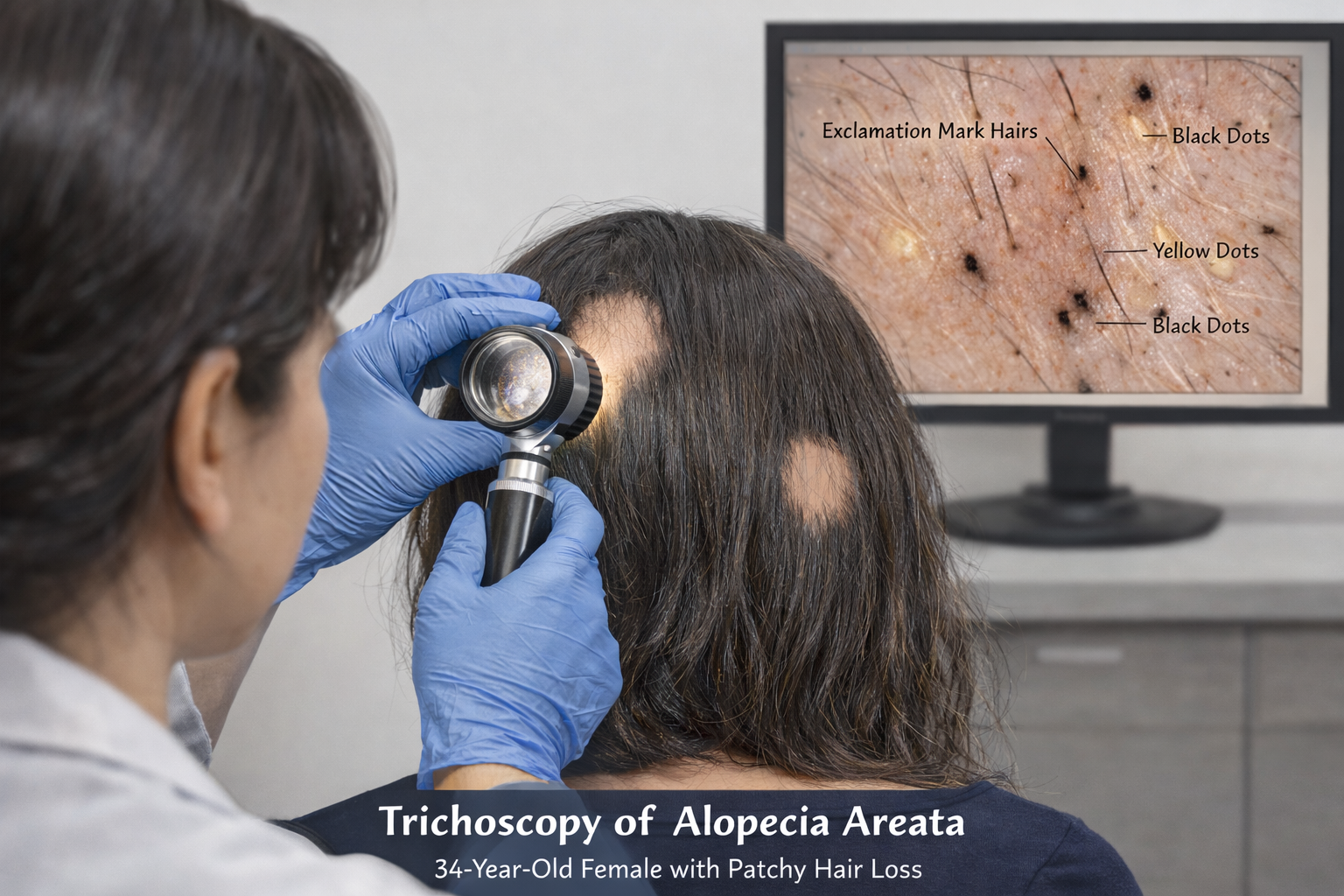
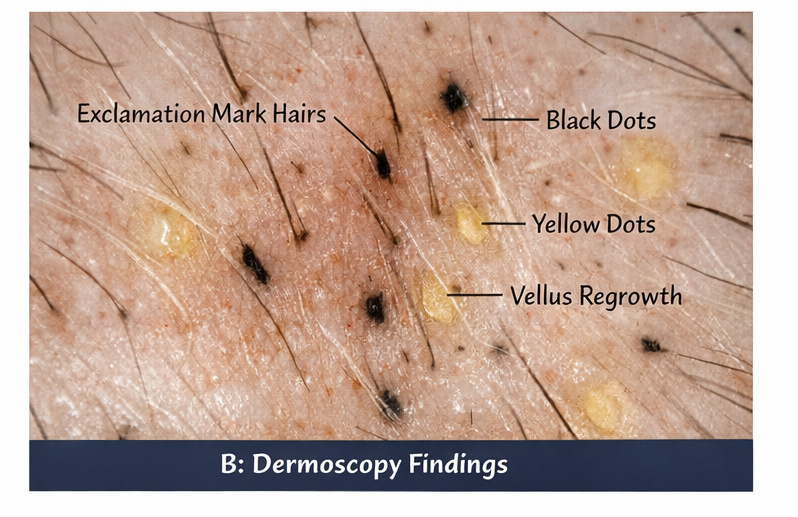
Trichoscopic evaluation revealed:
• Yellow dots
• Black dots
• Broken hairs
• Exclamation mark hairs
• Short vellus regrowing hairs
These findings supported active alopecia areata.
Laboratory Investigations
Routine hematological and biochemical parameters were within normal limits.
Thyroid function tests showed euthyroid status under treatment.
Autoimmune screening revealed no additional abnormalities. Serum ferritin and vitamin D levels were mildly reduced.
Fungal examination (KOH mount) was negative.
Based on clinical and dermoscopic findings, a diagnosis of patchy alopecia areata was established. Scalp biopsy was not performed as clinical findings were classical.
Management and Outcome
Treatment Planning
Given limited scalp involvement (<25% surface area) and absence of rapid progression, localized therapy was initiated. The patient was counseled regarding the autoimmune nature of the disease, unpredictable course, possibility of recurrence, and treatment expectations.
Psychological reassurance was emphasized due to visible cosmetic impact.
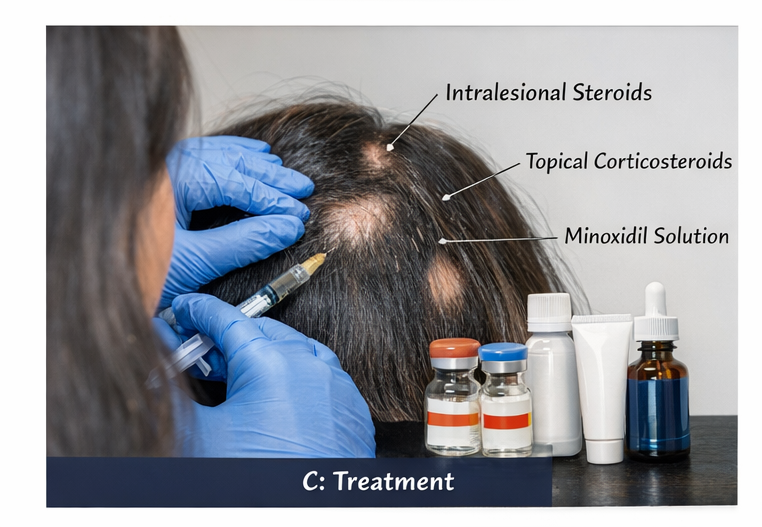
Medical Management
The patient received:
• Intralesional triamcinolone acetonide injections (5 mg/mL) every 4 weeks
• Topical corticosteroid lotion applied once daily
• Topical 5% minoxidil solution twice daily
• Vitamin D supplementation
Thyroid management was continued as per endocrinology advice.
Follow-Up and Outcome
At 8-week follow-up, early regrowth of fine vellus hairs was noted within treated patches. Hair pull test became negative.
At 3 months, significant terminal hair regrowth was observed in two patches, with partial regrowth in the third. No new lesions developed.
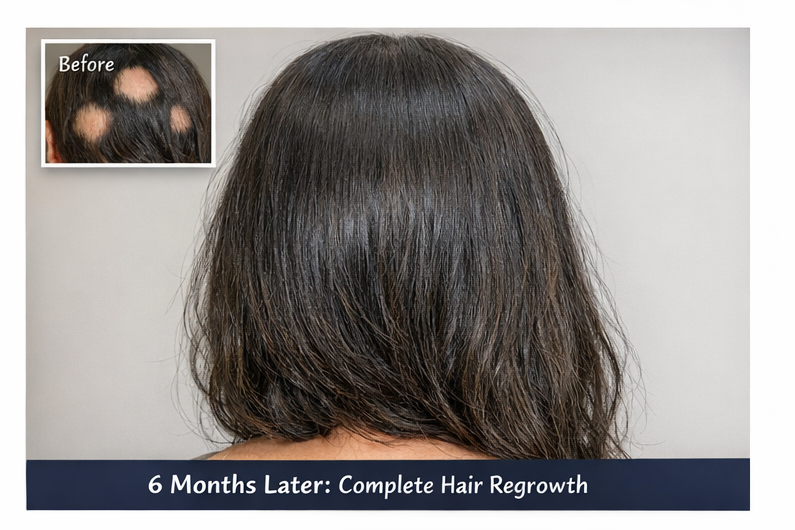
At 6 months, near-complete regrowth was achieved in all affected areas. Nail pitting persisted but did not worsen.
The patient reported improved confidence and reduced psychological distress.
At 12-month follow-up, the patient experienced a small recurrence in a new area (1 cm patch), which responded promptly to repeat intralesional therapy.
Overall, disease remained controlled with localized management.
Discussion
Alopecia areata is an immune-mediated disorder characterized by T-cell–mediated attack on hair follicles. Genetic predisposition and association with autoimmune diseases increase risk.
The hallmark clinical presentation includes sudden onset of well-defined, non-scarring alopecia patches. Exclamation mark hairs and nail pitting are important diagnostic clues.
Trichoscopy significantly enhances diagnostic accuracy, reducing need for biopsy in typical cases.
Management strategies depend on extent and severity:
- Localized disease: intralesional corticosteroids remain first-line therapy.
- Extensive disease: systemic corticosteroids, methotrexate, cyclosporine, or JAK inhibitors may be considered.
- Recent therapeutic advances include JAK inhibitors such as baricitinib, which have demonstrated efficacy in severe alopecia areata.
Despite therapeutic advances, the disease course remains unpredictable. Early treatment improves cosmetic outcomes and may reduce chronicity. Psychological support is integral due to the substantial impact on quality of life.
Conclusion
Alopecia areata is a chronic autoimmune hair disorder with significant psychosocial implications. Early recognition through clinical examination and dermoscopy allows timely intervention. Intralesional corticosteroids remain effective for localized disease, while emerging targeted therapies offer hope for extensive cases. Long-term follow-up is essential due to potential recurrence. Comprehensive management should address both medical and psychological aspects to optimize patient outcomes.
References
- Strazzulla LC, Wang EHC, Avila L, et al. Alopecia areata: An appraisal of new treatment approaches. J Am Acad Dermatol. 2018 https://pubmed.ncbi.nlm.nih.gov/29233618/
- Pratt CH, King LE Jr, Messenger AG, et al. Alopecia areata. Nat Rev Dis Primers. 2017. https://pubmed.ncbi.nlm.nih.gov/28696445/
- Messenger AG, McKillop J, Farrant P, et al. British Association of Dermatologists’ guidelines for the management of alopecia areata. Br J Dermatol. 2012. https://pubmed.ncbi.nlm.nih.gov/22524375/
- Alkhalifah A, Alsantali A, Wang E, et al. Alopecia areata update. J Am Acad Dermatol. 2010. https://pubmed.ncbi.nlm.nih.gov/20159338/
- King B, Ohyama M, Kwon O, et al. Two phase 3 trials of baricitinib for alopecia areata. N Engl J Med. 2022 https://pubmed.ncbi.nlm.nih.gov/35353990/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Researchers find distinct cell receptors with the potential for new treatments.
2.
Breast cancer patients' arms swell less after an effective lymph node transfer.
3.
Telehealth in the pandemic era resulted in fewer therapy interruptions.
4.
Too Many Chest CTs for Incidental Lung Nodules?
5.
Global warming could be driving up women's cancer risk, find researchers
1.
The New Frontier of Cancer Survivorship: Navigating the Long-Term Effects of Immunotherapy and Targeted Therapies
2.
Deterministic Reprogramming of Neutrophils within Tumors: A New Frontier in Cancer Research
3.
Neuroendocrine Tumors: Case Study on Diagnosis, Treatment Strategies & Patient Management
4.
Ticagrelor Monotherapy vs. Ticagrelor + Aspirin in ACS Post-PCI: ULTIMATE-DAPT Trial
5.
Transfusing the Future: Exploring the Possibilities of Blood Transfusions
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Current Scenario of Blood Cancer- A Conclusion on Genomic Testing & Advancement in Diagnosis and Treatment
2.
Navigating the Brain Barrier: The CNS Challenge in ALK+ NSCLC
3.
Thromboprophylaxis In Medical Settings
4.
Treatment Paradigm for Patients with R/R Adult B-cell ALL- Expert Discussions
5.
Current Scenario of Blood Cancer- Genomic Testing & Advancement in Diagnosis and Treatment

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge