Cushing Syndrome: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Cushing syndrome is an endocrine disorder characterized by prolonged exposure to elevated levels of glucocorticoids, either endogenous or exogenous in origin. It presents with a constellation of metabolic, dermatological, cardiovascular, and neuropsychiatric manifestations. The most common endogenous causes include adrenocorticotropic hormone (ACTH)-secreting pituitary adenomas (Cushing disease), adrenal tumors, and ectopic ACTH production. Patients often present with weight gain, central obesity, hypertension, glucose intolerance, and characteristic physical features such as moon facies and purple striae. Diagnosis involves biochemical confirmation of hypercortisolism followed by etiological localization using hormonal assays and imaging modalities. This case report describes a 38-year-old female presenting with classical features of Cushing syndrome due to a pituitary adenoma. It highlights the clinical presentation, diagnostic workup, management strategy, and favorable postoperative outcome.
Introduction
Cushing syndrome refers to the clinical state resulting from chronic exposure to excessive cortisol levels. It may arise from endogenous overproduction or exogenous administration of glucocorticoids. Endogenous causes are broadly categorized into ACTH-dependent and ACTH-independent etiologies.
ACTH-dependent causes include pituitary adenomas (Cushing disease) and ectopic ACTH secretion, whereas ACTH-independent causes include adrenal adenomas, carcinomas, or hyperplasia. The condition is associated with significant morbidity due to metabolic derangements, cardiovascular complications, and immunosuppression.
Early recognition is crucial, as untreated Cushing syndrome can lead to severe complications, including diabetes mellitus, osteoporosis, and increased mortality. Advances in biochemical testing and imaging techniques have significantly improved diagnostic accuracy and treatment outcomes.
Case Report
Patient History
A 38-year-old female presented to the endocrinology clinic with complaints of progressive weight gain over the past 10 months, predominantly around the abdomen and face. She also reported fatigue, muscle weakness, and irregular menstrual cycles.
The patient noted the development of reddish-purple stretch marks over her abdomen and thighs and increased facial hair growth. She also complained of mood swings and difficulty sleeping.
Her medical history was significant for hypertension diagnosed 6 months earlier, for which she was on antihypertensive therapy. There was no history of long-term corticosteroid use, ruling out exogenous causes.
There was no family history of endocrine disorders.
Clinical Examination
General Examination
- Central obesity with thin extremities
- Rounded “moon face” appearance
- Dorsocervical fat pad (“buffalo hump”)
- Facial hirsutism and acne
Vital Signs
- Blood pressure: 150/95 mmHg
- Pulse: 82/min
Skin Examination
- Wide, violaceous striae over abdomen
- Thin, fragile skin with easy bruising
Musculoskeletal System
- Proximal muscle weakness (difficulty rising from sitting position)
Clinical Evaluation
Differential Diagnosis
Based on clinical features, the following were considered:
- Cushing syndrome (endogenous)
- Polycystic ovary syndrome (PCOS)
- Metabolic syndrome
- Hypothyroidism
Given the characteristic features such as striae, muscle weakness, and hypertension, Cushing syndrome was strongly suspected.
Investigations
Initial Biochemical Tests
- 24-hour Urinary Free Cortisol (UFC)
- Elevated (3 times above normal range)
- Late-Night Salivary Cortisol
- Elevated, indicating loss of diurnal rhythm
- Low-Dose Dexamethasone Suppression Test (LDDST)
- No suppression of cortisol levels
These findings confirmed hypercortisolism.
Etiological Evaluation
- Plasma ACTH Levels
- Elevated → Suggesting ACTH-dependent Cushing syndrome
- High-Dose Dexamethasone Suppression Test (HDDST)
- Partial suppression of cortisol levels
- Suggestive of pituitary origin
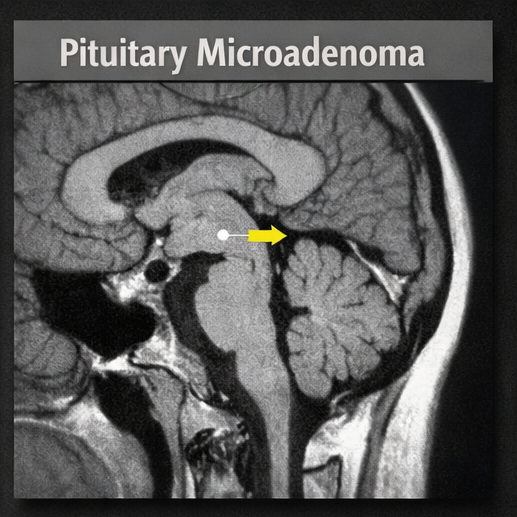
Imaging Studies
Magnetic Resonance Imaging (MRI) of the Brain
- Revealed a 6 mm pituitary microadenoma
CT Scan of Abdomen
- Normal adrenal glands
These findings confirmed a diagnosis of Cushing disease (pituitary adenoma).
Diagnosis
ACTH-dependent Cushing syndrome due to a pituitary microadenoma (Cushing disease)
Management and Outcome
Treatment Plan
Surgical Intervention
- The patient underwent transsphenoidal resection of the pituitary adenoma

Postoperative Management
- Temporary glucocorticoid replacement therapy
- Monitoring of serum cortisol levels
- Blood pressure and glucose control
Follow-Up and Clinical Progress
4 Weeks Post-Surgery
- Significant reduction in blood pressure
- Improved energy levels
- Cortisol levels reduced to near-normal
3 Months Post-Surgery
- Weight reduction of 5 kg
- Resumption of normal menstrual cycles
- Reduction in facial fullness
6 Months Post-Surgery
- Normal cortisol levels
- Resolution of hypertension
- Significant fading of striae
- Improved muscle strength

The patient demonstrated a favorable outcome with surgical management.
Discussion
Cushing syndrome represents a complex endocrine disorder with multisystem involvement. The pathophysiology revolves around chronic exposure to elevated cortisol levels, leading to metabolic dysregulation and tissue catabolism.
Pathophysiology
Excess cortisol results in:
- Increased gluconeogenesis → Hyperglycemia
- Protein catabolism → Muscle wasting
- Fat redistribution → Central obesity
- Suppression of immune response
- Mineralocorticoid effects → Hypertension
In ACTH-dependent cases, excessive ACTH stimulates adrenal cortisol production.
Etiology and Risk Factors
Endogenous Causes
- Pituitary adenoma (most common)
- Ectopic ACTH secretion (e.g., lung tumors)
- Adrenal tumors
Exogenous Causes
- Prolonged corticosteroid therapy
Risk Factors
- Female gender
- Chronic stress
- Hypertension
Clinical Features
- Central obesity
- Moon face
- Buffalo hump
- Purple striae
- Hypertension
- Hyperglycemia
- Osteoporosis
- Menstrual irregularities
- Psychiatric symptoms
Diagnostic Approach
Diagnosis requires a stepwise evaluation:
- Confirm hypercortisolism
- 24-hour urinary cortisol
- Salivary cortisol
- Dexamethasone suppression tests
- Determine cause
- ACTH levels
- High-dose suppression test
- Localization
- MRI (pituitary)
- CT (adrenal glands)
Management Strategies
1. Surgical Treatment
- First-line for pituitary adenomas
- High success rates
2. Medical Therapy
Used when surgery is contraindicated or incomplete:
- Ketoconazole
- Metyrapone
- Mitotane
3. Radiation Therapy
- For persistent or recurrent disease
Complications and Prognosis
Potential Complications
- Diabetes mellitus
- Cardiovascular disease
- Osteoporosis
- Infections
- Psychiatric disorders
Prognosis
- Good with early diagnosis and treatment
- Untreated cases have high morbidity and mortality
Conclusion
Cushing syndrome is a serious and potentially life-threatening endocrine disorder that necessitates a high index of clinical suspicion for timely and accurate diagnosis. Its presentation can often be subtle in the early stages, with nonspecific symptoms such as fatigue, weight gain, and mood disturbances, which may delay recognition. This case underscores the critical importance of identifying classical clinical features—including central obesity, facial rounding, proximal muscle weakness, hypertension, and characteristic skin changes such as violaceous striae—and correlating them with biochemical findings. A structured and systematic diagnostic approach, incorporating screening tests for hypercortisolism followed by confirmatory and localization studies, is essential to differentiate between various etiologies and guide appropriate management.
Pituitary adenoma, as seen in this case, remains the most common cause of endogenous Cushing syndrome (Cushing disease), and early identification significantly improves patient outcomes. Transsphenoidal surgical resection continues to be the first-line treatment and is associated with high success rates, particularly in cases of microadenomas. However, even after successful intervention, patients require careful and long-term follow-up due to the risk of recurrence and the persistence of metabolic complications such as hypertension, glucose intolerance, and osteoporosis.
Furthermore, comprehensive postoperative care, including hormonal monitoring, management of comorbidities, and patient education, plays a vital role in ensuring sustained recovery and improved quality of life. This case reinforces the need for a multidisciplinary approach involving endocrinologists, neurosurgeons, and primary care providers to optimize outcomes. Early diagnosis, timely intervention, and vigilant follow-up together form the cornerstone of effective management in Cushing syndrome.
References
- Nieman LK, et al. The diagnosis of Cushing's syndrome: An Endocrine Society Clinical Practice Guideline https://pubmed.ncbi.nlm.nih.gov/18334580/
- Lacroix A, et al. Cushing's syndrome https://pubmed.ncbi.nlm.nih.gov/25938990/
- Newell-Price J, et al. Cushing's syndrome https://pubmed.ncbi.nlm.nih.gov/12186730/
- Pivonello R, et al. The treatment of Cushing's disease https://pubmed.ncbi.nlm.nih.gov/28198966/
- Sharma ST, Nieman LK. Cushing’s syndrome: all variants, detection, and treatment https://pubmed.ncbi.nlm.nih.gov/29025524/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Electronic Sepsis Alerts; Reducing Plaques in Coronary Arteries
2.
Ivonescimab Tops Pembrolizumab in PD-L1-Positive, Advanced NSCLC
3.
Hereditary cancer has a rare and underreported cause.
4.
New imaging guidelines for head and neck cancers, a step toward practice change
5.
BMTs that are "half-matched" are effective in treating severe sickle cell disease.
1.
Oncolytic Adenoviruses Targeting PD-L1: Advancing Cancer Immunotherapy and Tumor Control
2.
Personalized Cancer Vaccines: The Next Frontier in Precision Oncology
3.
Essential Updates in Hematology in Daily Practice
4.
The Predictive Power of Theranostics in Palliative Neuroendocrine Tumor Management
5.
Importance of Early Detection in Oncology
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part VII
2.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part I
3.
Current Scenario of Cancer- The Incidence of Cancer in Men
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
A New Era in Managing Cancer-Associated Thrombosis

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge