Trigeminal Neuralgia: Clinical Presentation, Diagnostic Evaluation, Management, and Outcomes – A Case Report
OthersPage Navigation
Abstract
Trigeminal neuralgia is a chronic neuropathic pain disorder characterized by recurrent episodes of severe, sudden, electric shock-like facial pain along the distribution of the trigeminal nerve. It is considered one of the most painful neurological conditions and can significantly impair quality of life. The condition commonly affects individuals above 50 years of age and is often associated with neurovascular compression of the trigeminal nerve root.
We present the case of a 56-year-old female who presented with recurrent episodes of severe right-sided facial pain involving the maxillary and mandibular divisions of the trigeminal nerve. The pain was triggered by chewing, speaking, and brushing teeth. Neurological examination was otherwise normal. MRI brain with trigeminal nerve protocol excluded secondary causes and demonstrated vascular compression of the trigeminal nerve. The patient was treated with carbamazepine with significant symptomatic improvement.
This case highlights the importance of early recognition of trigeminal neuralgia, differentiation from dental and other facial pain disorders, and timely initiation of appropriate therapy to improve patient outcomes and quality of life.
Introduction
Trigeminal neuralgia (TN), also known as tic douloureux, is a neuropathic pain syndrome involving the fifth cranial nerve. The disorder is characterized by sudden, unilateral, recurrent episodes of severe facial pain lasting from a few seconds to minutes. The pain is commonly described as stabbing, lancinating, or electric shock-like.
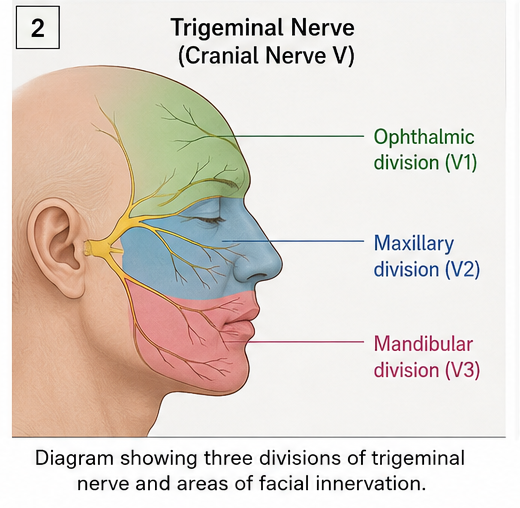
The trigeminal nerve provides sensory innervation to the face through three divisions:
- Ophthalmic (V1)
- Maxillary (V2)
- Mandibular (V3)
Trigeminal neuralgia most commonly affects the maxillary and mandibular divisions. The condition is usually unilateral and rarely bilateral.
The most common mechanism involves vascular compression at the trigeminal nerve root entry zone, resulting in focal demyelination and abnormal neuronal excitability. Secondary causes include multiple sclerosis, tumors, vascular malformations, and cerebellopontine angle lesions.
The annual incidence of trigeminal neuralgia is estimated to be approximately 4–13 cases per 100,000 individuals, with a higher prevalence among females and older adults.
Patients often experience severe pain triggered by otherwise harmless activities such as:
- Chewing
- Talking
- Brushing teeth
- Washing the face
- Cold wind exposure
Prompt diagnosis and early treatment are essential to reduce morbidity and improve quality of life.
Case Report
Patient History
A 56-year-old female presented to the neurology outpatient department with:
- Recurrent episodes of severe right-sided facial pain for 6 months
- Sudden electric shock-like pain over the cheek and jaw
- Pain lasting for a few seconds to 1 minute
- Multiple attacks occurring daily
- Triggering during chewing, brushing teeth, and speaking
The patient reported progressive worsening in frequency and severity of pain episodes.
There was no history of:
- Facial weakness
- Hearing loss
- Visual disturbances
- Fever
- Trauma
- Dental infection
Medical history revealed:
- Hypertension for 8 years
- No diabetes mellitus
- No previous neurological illness
Family history was non-contributory.
Clinical Examination
General Examination
- Patient conscious and oriented
- Blood pressure: 132/84 mmHg
- Pulse rate: 76/min
- Afebrile
- Systemic examination unremarkable
Neurological Examination
Cranial Nerve Examination
- Severe tenderness over right maxillary region during pain episodes
- Trigger zone identified near right nasolabial fold
- Facial sensations preserved
- Corneal reflex intact
- No facial muscle weakness
- No hearing deficits
Motor Examination
- Normal muscle tone and power
- No focal neurological deficit
Cerebellar Examination
- Normal
Meningeal Signs
- Absent
Clinical Evaluation
Differential Diagnosis
Based on history and examination, the following conditions were considered:
- Trigeminal neuralgia
- Dental pain
- Temporomandibular joint dysfunction
- Cluster headache
- Post-herpetic neuralgia
- Migraine
- Sinusitis
The characteristic episodic electric shock-like pain with trigger zones strongly suggested trigeminal neuralgia.
Investigations
Routine Laboratory Tests
- Complete blood count: Normal
- Blood glucose: Normal
- Renal function tests: Normal
- Liver function tests: Normal
MRI Brain with Trigeminal Nerve Protocol
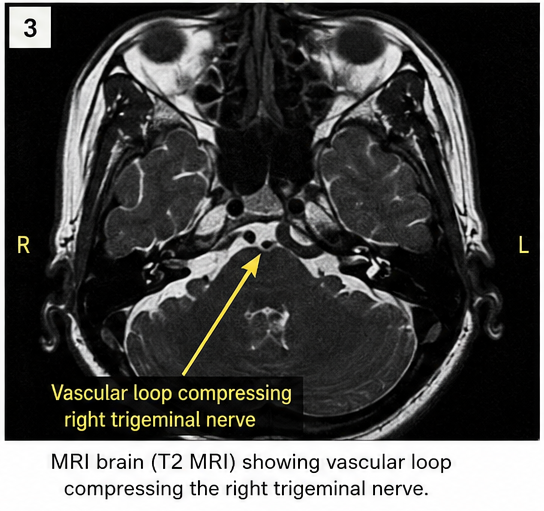
Findings included:
- Vascular loop compressing the right trigeminal nerve root entry zone
- No intracranial mass lesion
- No demyelinating plaques
- No cerebellopontine angle tumor
Dental Evaluation
- No dental abscess
- No significant dental pathology
Diagnosis
Based on clinical features and imaging findings, a diagnosis of:
Classical Trigeminal Neuralgia involving the right maxillary (V2) and mandibular (V3) divisions
was established.
Management and Outcome
Treatment Strategy
The goals of management included:
- Reduction of pain frequency
- Prevention of recurrent attacks
- Improvement in quality of life
- Long-term symptom control
Medical Management
The patient was started on:
- Carbamazepine 100 mg twice daily
- Gradual dose escalation based on response
- Vitamin supplementation
- Counseling regarding trigger avoidance
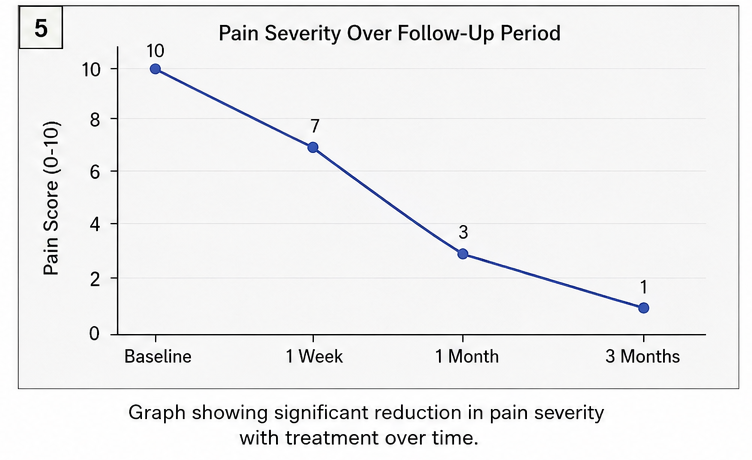
Clinical Course
At 1 Week
- Mild reduction in pain frequency
- Improved oral intake
At 1 Month
- Significant reduction in pain severity
- Only occasional breakthrough episodes
- Improved sleep and daily activities
At 3 Months
- Marked symptomatic improvement
- Minimal pain attacks
- Good drug tolerance
- No neurological deficits
Discussion
Pathophysiology
Trigeminal neuralgia commonly results from vascular compression of the trigeminal nerve root by adjacent arteries or veins. Chronic pulsatile compression leads to focal demyelination and hyperexcitability of trigeminal sensory fibers.
This results in:
- Abnormal ectopic impulse generation
- Ephaptic transmission between nerve fibers
- Severe paroxysmal facial pain
Secondary trigeminal neuralgia may occur due to:
- Multiple sclerosis
- Brain tumors
- Vascular malformations
- Cerebellopontine angle lesions
Epidemiology
- Incidence: 4–13 per 100,000 population annually
- More common in females
- Peak incidence after 50 years
- Right-sided involvement more common
- Bilateral involvement rare
Clinical Manifestations
Typical Symptoms
- Sudden electric shock-like facial pain
- Unilateral involvement
- Brief recurrent episodes
- Triggered by light touch or facial movements
Trigger Factors
- Chewing
- Speaking
- Brushing teeth
- Shaving
- Cold breeze exposure
Commonly Involved Divisions
- Maxillary division (V2)
- Mandibular division (V3)
Diagnostic Considerations
Diagnosis is primarily clinical and supported by imaging.
Important diagnostic tools include:
- Detailed pain history
- Neurological examination
- MRI brain with trigeminal nerve protocol
- Exclusion of dental and ENT causes
MRI is important to identify secondary causes and vascular compression.
Treatment Modalities
Medical Therapy
First-line medications include:
- Carbamazepine
- Oxcarbazepine
Other agents:
- Gabapentin
- Baclofen
- Lamotrigine
Surgical Options
Indicated in refractory cases:
- Microvascular decompression
- Radiofrequency rhizotomy
- Gamma knife radiosurgery
- Balloon compression
Microvascular decompression provides long-term pain relief in selected patients.
Complications
Potential complications include:
- Chronic debilitating pain
- Anxiety and depression
- Weight loss due to fear of eating
- Medication adverse effects
- Reduced quality of life
Untreated trigeminal neuralgia can significantly impair psychosocial functioning.
Prognosis
The prognosis depends on:
- Early diagnosis
- Response to medical therapy
- Presence of secondary causes
- Duration of symptoms
Most patients initially respond well to carbamazepine therapy. Surgical interventions offer favorable outcomes in medically refractory cases.
In this case, early treatment resulted in substantial symptomatic improvement and restoration of daily functioning.
Conclusion
Trigeminal neuralgia is a severely painful neuropathic facial pain disorder that requires prompt recognition and appropriate management. This case emphasizes the importance of identifying characteristic clinical features such as unilateral electric shock-like facial pain and trigger zones.
MRI evaluation is essential to exclude secondary causes and identify neurovascular compression. Early initiation of anticonvulsant therapy can significantly improve symptoms and quality of life.
Comprehensive clinical evaluation and individualized treatment remain the cornerstone of effective management in trigeminal neuralgia.
References
- Cruccu G, Finnerup NB, Jensen TS, et al. Trigeminal neuralgia: New classification and diagnostic grading. https://pubmed.ncbi.nlm.nih.gov/25344516/
- Maarbjerg S, Di Stefano G, Bendtsen L, Cruccu G. Trigeminal neuralgia – diagnosis and treatment. https://pubmed.ncbi.nlm.nih.gov/29290580/
- Zakrzewska JM, Linskey ME. Trigeminal neuralgia. https://pubmed.ncbi.nlm.nih.gov/18768918/
- Burchiel KJ. A new classification for facial pain. https://pubmed.ncbi.nlm.nih.gov/11844256/
- Gronseth G, Cruccu G, Alksne J, et al. Practice parameter: The diagnostic evaluation and treatment of trigeminal neuralgia. https://pubmed.ncbi.nlm.nih.gov/18721143/
- National Institute of Neurological Disorders and Stroke. Trigeminal Neuralgia Information Page. https://www.ninds.nih.gov/
- American Association of Neurological Surgeons. Trigeminal Neuralgia Overview. https://www.aans.org/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Novel ADC Improves Survival in Metastatic TNBC
2.
An Examine More Into the Acceptance of CRISPR/Cas9 Gene Therapy for Sickle Cell Illness.
3.
Celebrity Cancers Stoking Fear? Cisplatin Shortage Ends; Setback for Anti-TIGIT
4.
Pancreatic cancer RNA vaccine shows durable T cell immunity
5.
Healthcare in the Mix in President Biden's Farewell Address
1.
Interpreting Iron Studies: What Your Blood Results Really Mean
2.
Unveiling New Hope: Potential Therapeutic Targets in Hematological Malignancies
3.
Feline Anemia: Diagnosis and Treatment with Focus on Rasburicase Complications
4.
Andexanet for Factor Xa Inhibitor-Associated Acute Intracerebral Hemorrhage
5.
Biologic Therapies for Cutaneous Immune-Related Adverse Events in the Era of Immune Checkpoint Inhibitors
1.
Asian Symposium on Advancement in Hematology and Oncology
2.
Asian Symposium on Advancement in Hematology and Oncology
3.
Asian Symposium on Advancement in Hematology and Oncology
4.
International Cancer Conference
5.
Asian Symposium on Advancement in Hematology and Oncology
1.
Redefining Treatment Pathways in Relapsed/Refractory Adult B-Cell ALL
2.
Breaking Down PALOMA-2: How CDK4/6 Inhibitors Redefined Treatment for HR+/HER2- Metastatic Breast Cancer
3.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part I
4.
Cost Burden/ Burden of Hospitalization For R/R ALL Patients
5.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part VI

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge