Dry Gangrene: Clinical Evaluation, Multidisciplinary Management, and Outcome - A Case Report
OthersPage Navigation
Abstract
Dry gangrene is a form of ischemic tissue necrosis resulting from chronic arterial insufficiency, most commonly associated with long-standing diabetes mellitus and peripheral arterial disease. It is characterized by dry, shriveled, and mummified tissue with a clear line of demarcation and absence of active infection. Early recognition and accurate differentiation from wet gangrene are critical, as management strategies and prognostic implications differ significantly. We report a case of dry gangrene of the foot in an elderly male with diabetes and peripheral vascular disease. Comprehensive clinical evaluation, vascular imaging, metabolic optimization, and a staged multidisciplinary approach led to definitive surgical management with favorable outcomes. This case underscores the importance of timely diagnosis, vascular assessment, and coordinated care in preventing systemic complications and optimizing limb outcomes.
Introduction
Gangrene refers to tissue necrosis resulting from compromised blood supply, infection, or a combination of both. Dry gangrene is typically caused by chronic ischemia due to progressive atherosclerotic occlusion of peripheral arteries and is most frequently encountered in patients with diabetes mellitus, peripheral arterial disease, smoking history, and advanced age [1]. Unlike wet gangrene, dry gangrene is not associated with acute infection or systemic toxicity and progresses slowly.
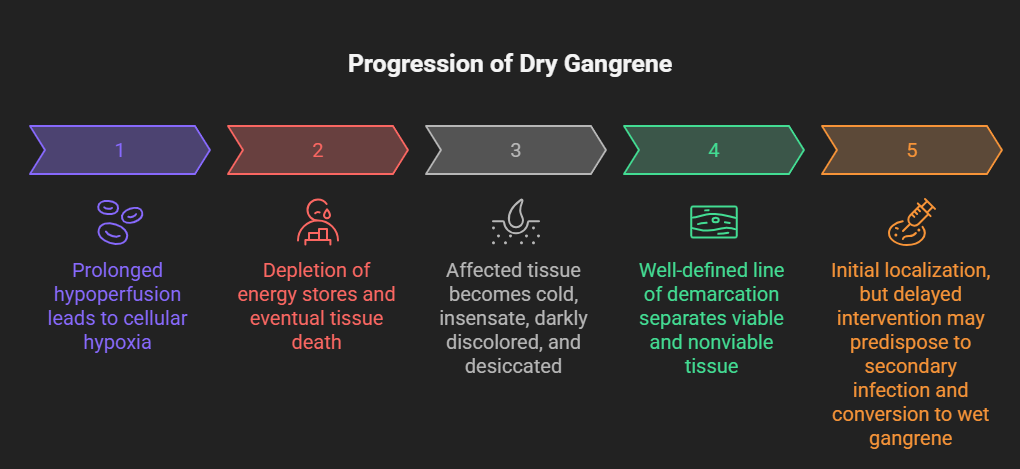
Pathophysiologically, prolonged hypoperfusion leads to cellular hypoxia, depletion of energy stores, and eventual tissue death. The affected tissue becomes cold, insensate, darkly discolored, and desiccated, often with a well-defined line of demarcation separating viable and nonviable tissue [2]. Although dry gangrene is initially localized, delayed intervention may predispose to secondary infection and conversion to wet gangrene, significantly increasing morbidity and mortality.
Early diagnosis, thorough vascular assessment, and appropriate surgical planning are essential to preserve limb function and prevent life-threatening complications. This case report describes the clinical presentation, diagnostic workup, and management of dry gangrene, highlighting key principles of contemporary care.
Case Report
Patient History
A 64-year-old male presented to the general surgery outpatient department with progressive black discoloration of the toes of the left foot for three weeks.
The patient reported associated numbness and coldness of the affected toes but denied pain, discharge, fever, or foul odor. There was no history of trauma or recent infection. The patient had a 15-year history of type 2 diabetes mellitus with suboptimal glycemic control and a 10-year history of hypertension. He was a former smoker with a 25-pack-year history. There was no prior history of lower limb revascularization or amputations.
Clinical Examination
On general examination, the patient was hemodynamically stable and afebrile. Local examination of the left foot revealed dry, blackened, shriveled distal phalanges of the second and third toes with a clear line of demarcation at the level of the proximal interphalangeal joints. The surrounding skin was dry and atrophic, with no erythema, warmth, edema, or purulent discharge.

Peripheral pulses were diminished. The dorsalis pedis and posterior tibial pulses on the left side were not palpable, while the right-sided pulses were weakly palpable. Capillary refill was markedly delayed. Sensory examination revealed reduced protective sensation, consistent with diabetic peripheral neuropathy.
Investigations
Laboratory Studies
Baseline laboratory investigations revealed elevated fasting blood glucose and glycated hemoglobin (HbA1c 9.1%), indicating poor glycemic control. White blood cell count and inflammatory markers were within normal limits, supporting the absence of active infection. Renal and hepatic function tests were unremarkable.
Vascular Imaging
Doppler ultrasonography of the lower limbs demonstrated diffuse atherosclerotic changes with significantly reduced arterial flow in the left anterior tibial and posterior tibial arteries. Ankle–brachial index (ABI) on the left side was 0.45, consistent with severe peripheral arterial disease.

Computed tomography angiography (CTA) revealed multilevel arterial occlusion involving the superficial femoral artery with poor distal runoff, limiting the feasibility of revascularization.

Diagnosis
Based on clinical findings and vascular imaging, a diagnosis of dry gangrene of the left second and third toes secondary to chronic limb-threatening ischemia due to peripheral arterial disease was established.
Management and Outcome
Multidisciplinary Approach
The patient was managed jointly by general surgery, vascular surgery, endocrinology, and wound care teams. Initial management focused on metabolic optimization, including strict glycemic control, antihypertensive therapy, antiplatelet agents, and statins. The affected limb was kept dry and protected, with close monitoring for signs of infection.
Surgical Management
Given the presence of a well-demarcated dry gangrene and limited revascularization options, a decision was made to proceed with elective surgical amputation of the nonviable toes once demarcation was complete. The patient underwent left second and third toe amputation under regional anesthesia.
Intraoperatively, the proximal tissues appeared viable with minimal bleeding, confirming adequate demarcation. No purulent material or evidence of infection was noted.

Follow-Up and Outcome
Postoperative recovery was uneventful. The surgical wound healed by secondary intention with regular dressings and offloading measures. At six-week follow-up, the patient demonstrated satisfactory wound healing, improved mobility, and no progression of ischemia.
The patient was counseled extensively on foot care, smoking cessation, and adherence to medical therapy. Long-term follow-up with vascular and diabetic services was arranged to prevent recurrence and progression of disease.
Discussion
Dry gangrene represents the end stage of chronic ischemia and is a marker of advanced peripheral arterial disease. Diabetes mellitus plays a central role by accelerating atherosclerosis, impairing microcirculation, and reducing pain perception due to neuropathy, often leading to delayed presentation [3].
Differentiation between dry and wet gangrene is critical, as dry gangrene allows for planned surgical intervention, whereas wet gangrene constitutes a surgical emergency due to the risk of sepsis. Vascular imaging is essential to assess limb perfusion and determine revascularization potential [4].
In this case, severe multilevel arterial disease limited revascularization options, and timely amputation of nonviable tissue prevented secondary infection and systemic complications. Multidisciplinary management and patient education remain central to improving outcomes in such patients.
Conclusion
Dry gangrene is a serious manifestation of chronic peripheral ischemia requiring prompt recognition and structured management to prevent local progression and systemic complications. This case highlights the importance of comprehensive vascular assessment to accurately define the extent of arterial disease and determine the feasibility of revascularization, as well as meticulous metabolic optimization to address contributory factors such as poor glycemic control, hypertension, and dyslipidemia. Timely and appropriately planned surgical intervention, undertaken once clear demarcation is established, plays a crucial role in achieving optimal wound healing and functional outcomes. Early diagnosis and coordinated multidisciplinary care involving surgeons, vascular specialists, endocrinologists, and wound care teams are essential not only to prevent disease progression and limb loss, but also to reduce recurrence risk, enhance patient education, and ultimately improve long-term quality of life.
References
- Frykberg RG, Banks J. Challenges in the treatment of chronic wounds. Adv Wound Care. 2015;4(9):560–582.
- Norgren L, et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007;45(Suppl S):S5–S67.
- Hingorani A, et al. The management of diabetic foot: A clinical practice guideline. J Vasc Surg. 2016;63(2 Suppl):3S–21S.
- Conte MS, et al. Global vascular guidelines on the management of chronic limb-threatening ischemia. Eur J Vasc Endovasc Surg. 2019;58(1S):S1–S109.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Remote monitoring can improve recovery from cancer surgery
2.
Intractable cancers may respond better to treatment when using new radiation and high-performance computing.
3.
A Win for AI in Cancer; 2025's Transformative Drugs; FDA Clarifies 'Underway' Trials
4.
Conditional EU Nod for Weekly Pill in Pediatric Glioma
5.
high response rate when using a bispecific antibody to treat R/R multiple myeloma.
1.
The Technological Revolution in Precision Oncology and Tumor Microenvironment Therapy
2.
The Role of the Oncology Pharmacist: From Treatment to Trials and Beyond
3.
Unlocking the Secrets of Neutrophils: Exploring Their Role in Immune Defense
4.
New Hope for Rectal Cancer Patients: Breakthrough Drug Shows Promising Results
5.
Unveiling the Mystery of Echinocyte: A Closer Look at the Unique Red Blood Cell
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Role of Nimotuzumab in Management of Nasopharyngeal Cancer
2.
The Landscape of First-Line Treatment for Urothelial Carcinoma- The Conclusion
3.
Pazopanib Takes Center Stage in Managing Renal Cell Carcinoma - Part III
4.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part IV
5.
An Eagles View - Evidence-based Discussion on Iron Deficiency Anemia- Panel Discussion

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge