Situs Inversus Totalis: Clinical Presentation, Diagnostic Evaluation, and Outcome – A Case Report
OthersPage Navigation
Abstract
Situs inversus totalis is a rare congenital condition characterized by complete mirror-image transposition of thoracic and abdominal organs. The condition results from abnormal embryological rotation of the viscera during early development and has an estimated incidence of approximately 1 in 10,000 individuals. Most patients remain asymptomatic and are often diagnosed incidentally during imaging performed for unrelated conditions. However, recognition of this anatomical variation is clinically important because it may alter physical examination findings, diagnostic interpretation, and surgical planning. Associated anomalies such as congenital heart disease or primary ciliary dyskinesia may occur in a subset of patients. Diagnosis is typically confirmed through imaging modalities including chest radiography, ultrasonography, computed tomography (CT), and echocardiography. This case report describes a young adult male with incidentally detected situs inversus totalis during evaluation for abdominal pain, highlighting clinical findings, diagnostic workup, and clinical implications.
Introduction
Situs inversus totalis is a congenital anomaly in which the thoracic and abdominal organs are arranged in a complete mirror image of their normal anatomical positions. In this condition, the heart is located on the right side of the thorax (dextrocardia), the liver and gallbladder are situated on the left side of the abdomen, and the spleen and stomach are located on the right.
The condition arises due to disturbances in the normal left–right axis determination during embryogenesis. Although most individuals with situs inversus totalis have normal organ function and life expectancy, recognition of the condition is important because it can lead to diagnostic confusion during clinical evaluation. Symptoms of common diseases may present on the opposite side of the body, potentially delaying diagnosis.
In some patients, situs inversus totalis may be associated with primary ciliary dyskinesia, a condition known as Kartagener syndrome, which includes chronic sinusitis, bronchiectasis, and situs inversus. Imaging plays a key role in confirming the diagnosis and evaluating associated anomalies. This report presents a case of incidentally diagnosed situs inversus totalis during imaging evaluation.
Case Report
Patient History
A 26-year-old male presented to the outpatient department with complaints of intermittent abdominal discomfort for three days. The pain was mild, non-radiating, and not associated with nausea, vomiting, or fever. There was no history of trauma, previous abdominal surgery, or chronic medical illness.
The patient reported normal bowel and urinary habits. There was no history of respiratory symptoms such as chronic cough or recurrent sinus infections. Family history was unremarkable.
Clinical Examination
On examination, the patient appeared comfortable and hemodynamically stable.
• Temperature: 36.8°C
• Pulse: 78 beats per minute
• Blood pressure: 118/74 mmHg
• Respiratory rate: 16 breaths per minute
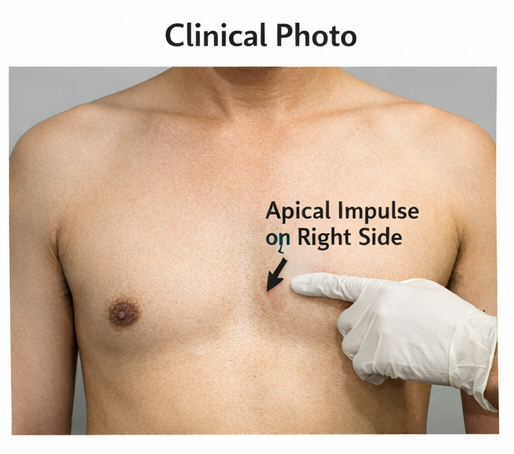
Cardiac examination revealed the apical impulse palpable in the right fifth intercostal space, raising suspicion of dextrocardia. Heart sounds were normal without murmurs.
Abdominal examination revealed mild tenderness in the left upper quadrant. The liver was not palpable in the right hypochondrium. No organomegaly or guarding was noted.
Clinical Evaluation
Differential Diagnosis
Based on the unusual physical findings, the following possibilities were considered:
• Dextrocardia with normal abdominal organ position
• Situs inversus totalis
• Congenital cardiac anomaly with displaced apex
• Technical error in examination findings
Further imaging studies were planned to clarify the anatomical arrangement.
Investigations
Laboratory Findings
Routine laboratory investigations were within normal limits.
• Hemoglobin: 13.6 g/dL
• Total leukocyte count: 6,200/mm³
• Platelet count: 210,000/mm³
• Liver function tests: Normal
• Renal function tests: Normal
No biochemical abnormalities were detected.
Imaging
Chest Radiograph
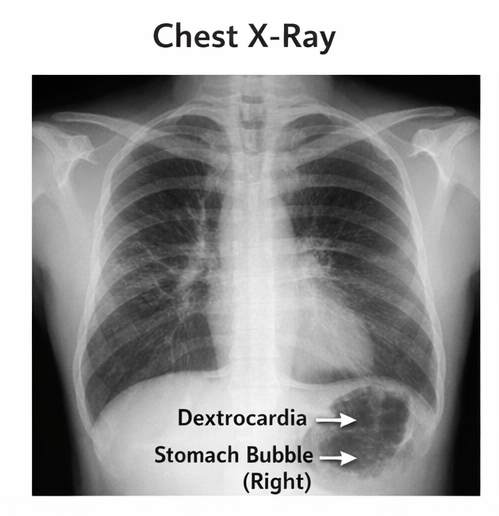
Chest X-ray revealed dextrocardia, with the cardiac apex directed toward the right side. The gastric air bubble was noted beneath the right hemidiaphragm, suggesting mirror-image abdominal organ positioning.
Ultrasound Abdomen
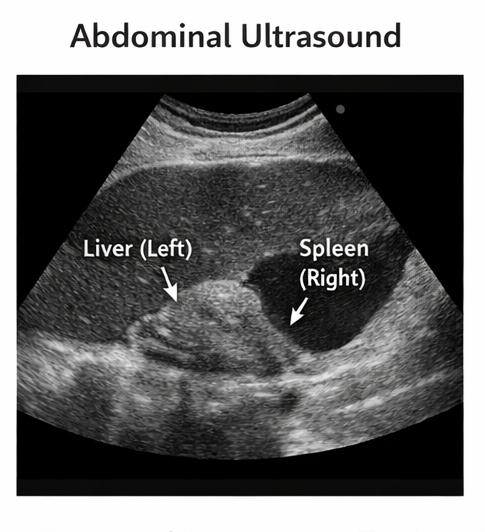
Abdominal ultrasonography demonstrated mirror-image arrangement of abdominal viscera. The liver and gallbladder were located in the left upper abdomen, while the spleen and stomach were located on the right side.
Computed Tomography (CT) Abdomen and Thorax
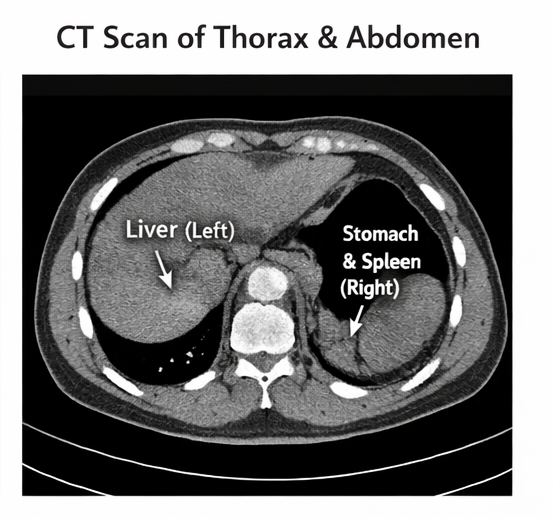
Contrast-enhanced CT confirmed complete transposition of thoracic and abdominal organs, including right-sided stomach and spleen and left-sided liver and inferior vena cava. The heart was located on the right side with a right-sided aortic arch orientation consistent with dextrocardia.
No structural abnormalities of abdominal organs were identified.
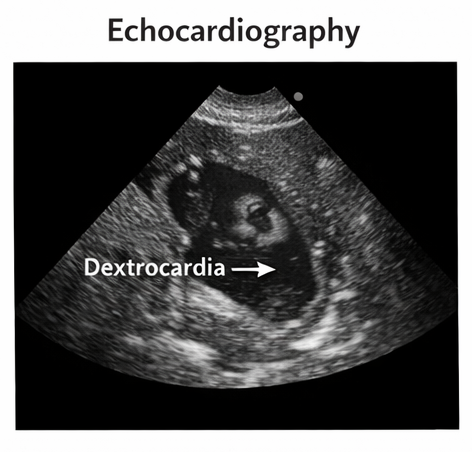
Echocardiography
Echocardiographic evaluation confirmed dextrocardia with structurally normal cardiac chambers and valves, with no evidence of congenital heart disease.
Diagnosis
Based on clinical examination and imaging findings, a diagnosis of situs inversus totalis with dextrocardia was established.
Management and Outcome
Clinical Management
As the patient had no functional abnormalities or associated cardiac defects, no specific treatment was required. The abdominal discomfort was attributed to mild gastritis and managed conservatively with dietary modification and symptomatic medication.
The patient was counseled regarding his anatomical variation and advised to inform healthcare providers about his condition in future medical encounters to avoid diagnostic confusion.
Follow-Up and Outcome
At follow-up after two weeks, the patient reported complete resolution of abdominal discomfort. He remained asymptomatic with normal daily functioning.
No further complications were noted, and long-term prognosis was considered excellent.
Discussion
Situs inversus totalis is a rare congenital anomaly resulting from abnormal rotation of visceral organs during embryonic development. The condition follows an autosomal recessive inheritance pattern in some cases, although many cases occur sporadically.
Most individuals with situs inversus totalis remain asymptomatic and lead normal lives. However, the condition may be discovered incidentally during imaging or during evaluation for unrelated symptoms.
Dextrocardia is a defining feature of situs inversus totalis. Approximately 3–5% of patients may have associated congenital heart disease, which is significantly lower compared with isolated dextrocardia without situs inversus.
Clinical recognition of this condition is important because common diseases may present with reversed symptom locations. For example, appendicitis may present with left lower quadrant pain rather than the typical right-sided pain.
Imaging modalities such as chest radiography, ultrasonography, and CT scanning are crucial for confirming organ orientation and excluding associated abnormalities. Echocardiography is recommended to assess for congenital cardiac defects.
Management generally involves patient education and documentation of the anatomical variation in medical records. Surgical procedures may require modification of standard approaches due to reversed anatomy.
Conclusion
Situs inversus totalis is an uncommon congenital condition characterized by mirror-image transposition of thoracic and abdominal organs. Most individuals remain asymptomatic and are diagnosed incidentally during imaging studies. Awareness of this anatomical variation is important to avoid diagnostic errors and to guide surgical or interventional procedures. Comprehensive imaging evaluation helps confirm the diagnosis and identify associated anomalies. With proper recognition and documentation, individuals with situs inversus totalis can lead normal and healthy lives.
References
- Maldjian PD, Saric M. Approach to dextrocardia in adults: review. Am Heart J. 2007. https://pubmed.ncbi.nlm.nih.gov/17584555/
- Bohun CM, Potts JE, Casey BM, Sandor GG. A population-based study of cardiac malformations in dextrocardia. Pediatr Cardiol. 2007. https://pubmed.ncbi.nlm.nih.gov/17111282/
- Shapiro AJ, Zariwala MA, Ferkol T, et al. Primary ciliary dyskinesia and situs abnormalities. Am J Respir Crit Care Med. 2016. https://pubmed.ncbi.nlm.nih.gov/27367784/
- Afzelius BA. A human syndrome caused by immotile cilia. Science. 1976. https://pubmed.ncbi.nlm.nih.gov/1084576/
- Applegate KE, Goske MJ, Pierce G, Murphy D. Situs revisited: imaging of the heterotaxy syndrome. Radiographics. 1999. https://pubmed.ncbi.nlm.nih.gov/10464797/
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Year in Review: Chronic Lymphocytic Leukemia
2.
According to a study, white Americans are overdiagnosing melanoma at an alarming rate.
3.
Approval in Endometrial Cancer Expanded; Masks at Cancer Centers; NPR Reporter Dies
4.
The First Gene Therapy Provides a Durable Response for Non-Muscle-Invasive Bladder Cancer.
5.
Canine Cancer Vaccine: A Potential Resurrection? U.S. KK. Snubs Enertu.
1.
What Is Carboxyhemoglobin And How Can It Affect Your Health?
2.
Lu-177 Vipivotide in Prostate Cancer: A Breakthrough in Radioligand Therapy
3.
Unraveling the Mysteries of Coagulopathy: A Comprehensive Definition
4.
Machine Learning in Genomic Analysis for Early Lung Cancer Detection: Key Advances and Insights
5.
A New Perspective on Spherocytosis: Uncovering Innovative Treatments
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Revolutionizing Treatment of ALK Rearranged NSCLC with Lorlatinib - Part II
2.
Navigating the Complexities of Ph Negative ALL - Part XIII
3.
Updates on the First Line Management of ALK+ NSCLC
4.
Untangling The Best Treatment Approaches For ALK Positive Lung Cancer - Part IV
5.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part II

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge