Ecchymosis: Clinical Evaluation, Multidisciplinary Management, and Outcome - A Case Report
OthersPage Navigation
Abstract
Ecchymosis refers to subcutaneous bleeding resulting in discoloration of the skin larger than 1 cm, commonly perceived as bruising. While often benign and trauma-related, ecchymosis may also signify underlying systemic disorders such as coagulopathies, platelet abnormalities, vascular fragility, or adverse drug effects. Clinical presentation ranges from isolated, self-limiting lesions to widespread bruising associated with serious hematological or systemic disease. Accurate diagnosis requires careful clinical history, physical examination, and targeted laboratory investigations to identify the underlying etiology. Management is primarily directed toward treating the underlying cause and preventing complications. We report a case of recurrent spontaneous ecchymosis in a middle-aged female, ultimately diagnosed with acquired platelet dysfunction secondary to antiplatelet therapy. A multidisciplinary approach involving internal medicine, hematology, and dermatology led to resolution of symptoms and prevention of recurrence. This case emphasizes the importance of thorough evaluation of ecchymosis to exclude serious systemic pathology.
Introduction
Ecchymosis is a common clinical finding characterized by extravasation of blood into subcutaneous tissues, producing non-blanching purplish discoloration of the skin. Unlike petechiae and purpura, ecchymoses are larger lesions and often result from trauma; however, spontaneous ecchymosis warrants careful investigation [1].
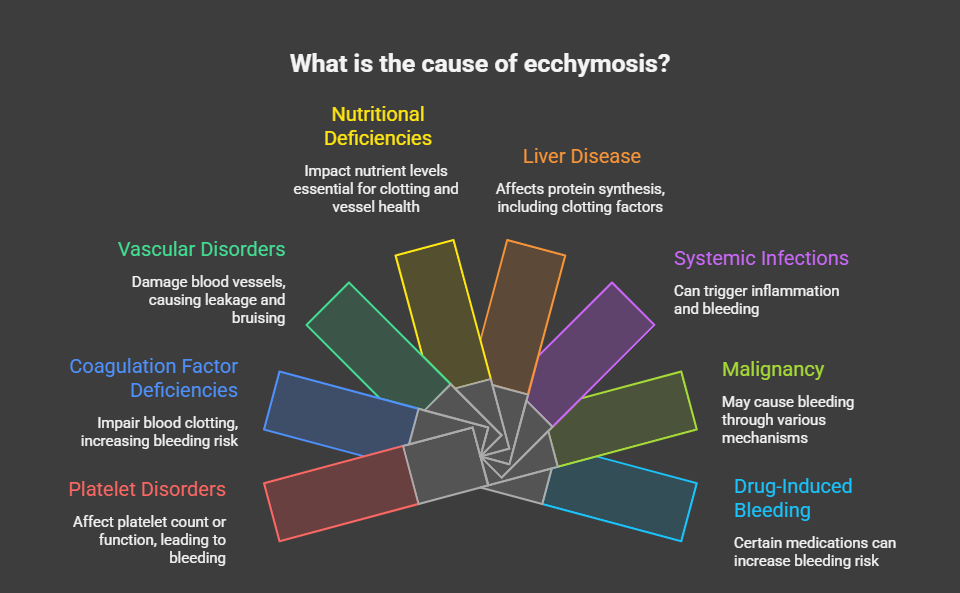
The differential diagnosis of ecchymosis is broad and includes platelet disorders, coagulation factor deficiencies, vascular disorders, nutritional deficiencies, liver disease, systemic infections, malignancy, and drug-induced bleeding tendencies [2]. Anticoagulants, antiplatelet agents, corticosteroids, and certain herbal supplements are frequently implicated.
Although many cases are benign, unexplained or recurrent ecchymosis may represent a manifestation of serious underlying disease. Early recognition, systematic evaluation, and multidisciplinary management are essential to prevent morbidity. This case report describes the clinical assessment, diagnostic workup, and management of spontaneous ecchymosis, highlighting the importance of identifying reversible causes.
Case Report
Patient History
A 46-year-old female presented to the general medicine clinic with complaints of recurrent bruising over her upper and lower limbs for two months. The bruises appeared spontaneously, without any history of trauma, and gradually changed color before resolving over 10–14 days. She denied associated pain, fever, weight loss, joint swelling, or bleeding from other sites such as gums, nose, or gastrointestinal tract.

The patient had a history of ischemic heart disease and had been on dual antiplatelet therapy (aspirin and clopidogrel) for the past one year. There was no personal or family history of bleeding disorders. She was not on anticoagulants, corticosteroids, or herbal medications.
Clinical Examination
On examination, the patient was hemodynamically stable and afebrile. Multiple ecchymotic patches measuring 3–6 cm were noted over the forearms and thighs. The lesions were non-tender, non-blanching, and in various stages of resolution. No petechiae or purpura were observed.
There was no pallor, icterus, lymphadenopathy, or hepatosplenomegaly. Joint examination was unremarkable, and systemic examination did not reveal any abnormal findings.
Investigations
Laboratory Studies
Complete blood count revealed normal hemoglobin levels, total leukocyte count, and platelet count. Peripheral smear showed normal platelet morphology. Coagulation profile including prothrombin time (PT), activated partial thromboplastin time (aPTT), and international normalized ratio (INR) were within normal limits.
Liver function tests, renal function tests, and inflammatory markers were normal. Bleeding time was mildly prolonged. Platelet function analysis suggested impaired platelet aggregation consistent with antiplatelet drug effect.
Diagnosis
Based on clinical findings and laboratory evaluation, a diagnosis of drug-induced ecchymosis secondary to antiplatelet therapy–associated platelet dysfunction was established.
Management and Outcome
Multidisciplinary Approach
The patient’s case was reviewed jointly by internal medicine, cardiology, hematology, and dermatology teams. The risks and benefits of continued dual antiplatelet therapy were carefully assessed in the context of her cardiovascular history and bleeding manifestations.

Therapeutic Management
Clopidogrel was temporarily discontinued after cardiology consultation, while aspirin was continued at a reduced dose. The patient was advised to avoid minor trauma, nonsteroidal anti-inflammatory drugs, and over-the-counter supplements that could exacerbate bleeding.
Vitamin C supplementation was initiated to support vascular integrity. The patient was reassured regarding the benign nature of the lesions once the underlying cause was identified.

Follow-Up
At four-week follow-up, no new ecchymotic lesions were observed. Existing bruises had completely resolved. Repeat platelet function testing showed improvement. The patient remained clinically stable and was continued on single antiplatelet therapy with close follow-up.
Discussion
Ecchymosis is a frequent but often underappreciated clinical sign that may reflect underlying hemostatic abnormalities. Drug-induced platelet dysfunction is a common and reversible cause, particularly in patients receiving antiplatelet agents for cardiovascular disease [3].
A structured diagnostic approach—including detailed medication history, laboratory evaluation, and multidisciplinary input—is critical to avoid unnecessary investigations and ensure patient safety. Differentiating benign causes from serious systemic conditions such as hematological malignancies or inherited bleeding disorders is essential [4].
Management focuses on correcting the underlying cause, modifying risk factors, and patient education. Most cases resolve once the precipitating factor is addressed, as demonstrated in this case.
Conclusion
Ecchymosis, although frequently perceived as a benign and self-limiting finding, can serve as a significant clinical indicator of underlying systemic disease or drug-related pathology when it occurs spontaneously or recurs without obvious trauma. Such presentations should prompt clinicians to conduct a thorough and structured clinical assessment, including detailed history-taking with emphasis on medication use, comorbid conditions, nutritional status, and family history of bleeding disorders. Targeted laboratory investigations are essential to identify platelet abnormalities, coagulation defects, or vascular fragility, and to exclude serious conditions such as hematological disorders or systemic illnesses.
This case underscores the importance of a multidisciplinary, patient-centered approach involving internists, hematologists, and other relevant specialists to ensure accurate diagnosis and individualized management. Collaborative decision-making enables appropriate modification of offending medications, optimization of underlying medical conditions, and implementation of preventive strategies. Early recognition and coordinated care not only lead to favorable clinical outcomes and symptom resolution but also help avoid unnecessary investigations, reduce patient anxiety, and minimize the risk of future bleeding complications.
References
- Rodeghiero F, Tosetto A. Clinical evaluation of bleeding and bruising. Hematology Am Soc Hematol Educ Program. 2013;2013:517–522.
- Kitchens CS, Kessler CM, Konkle BA. Consultative Hemostasis and Thrombosis. 3rd ed. Elsevier; 2013.
- Patrono C, et al. Antiplatelet drugs: mechanisms of action and clinical applications. J Am Coll Cardiol. 2017;70(14):1760–1776.
- Bolton-Maggs PHB. The investigation of bleeding disorders. Clin Med. 2015;15(3):252–256.
Read more such content on @ Hidoc Dr | Medical Learning App for Doctors
Recommended News For You
Recommended Articles For You
Featured News
Featured Articles
Featured Events
Featured KOL Videos
1.
Non-Factor Therapies in Hemophilia: Cutting-Edge Approaches to Individualize Care
2.
FDA approves Blenrep for relapsed or refractory multiple myeloma
3.
X-ray and radar technology combined to reduce cancer screening risks
4.
Extended Maintenance with Imatinib Enhances Disease-Free Survival in High-Risk GIST.
5.
Researchers discuss HER2-low and HER2-zero in breast cancer
1.
Understanding Mesenteric Masses: Symptoms, Diagnosis, and Treatment Options
2.
Liposomal Doxorubicin and Mitomycin in Modern Cancer Treatment
3.
The New Era of Oncology: Key Updates and Clinical Insights
4.
HIPEC in Platinum-Sensitive Ovarian Cancer: A Promising Yet Controversial Option
5.
Theranostics and Radioligand Therapy: Precision Cancer Care with Targeted Radionuclides
1.
International Lung Cancer Congress®
2.
Genito-Urinary Oncology Summit 2026
3.
Future NRG Oncology Meeting
4.
ISMB 2026 (Intelligent Systems for Molecular Biology)
5.
Annual International Congress on the Future of Breast Cancer East
1.
Exploring Potentials of Lorlatinib: The Third Generation ALK-TKI Through CROWN Trial
2.
Managing ALK Rearranged Non-Small Cell Lung Cancer with Lorlatinib - Part I
3.
Breaking Ground: ALK-Positive Lung Cancer Front-Line Management - Part V
4.
A Comprehensive Guide to First Line Management of ALK Positive Lung Cancer - Part II
5.
Expert Group meeting with the management of EGFR mutation positive NSCLC - Part III

Address :
Hidoc Dr. Inc. | Delaware C Corp | 1309 Coffeen Ave. Suite 1200, Sheridan WY, 82801
Phone :
+1-415-463-3094
Email :
anishagadia@hidoc.co
© Copyright 2026 Hidoc Dr. Inc.
Terms & Conditions - LLP | Inc. | Privacy Policy - LLP | Inc. | Account Deactivation

To get started please enter your email ID
Welcome to Hidoc Dr.
Join to enhance your clinical skills and gain specialized in-depth medical knowledge